Once you reach a ‘certain’ age, you are horrified, but not surprised to get a cancer diagnosis, or hear about it in a loved one. That same cancer in a young person is even more horrifying, we instinctively know.
Most kidney cancers (and there are more types than we previously knew) are found in people in their 60s and 70s. Bad enough, but a cancer called by the same name and found in a younger person is often a very different cancer, with a very different prognosis.
Some new research recognizes that special attention should be paid to those RCCs found in patients 46 years of age and younger. Why is this?
The quick answer is that this may represent a more aggressive kidney cancer and/or be of a familial or hereditary nature. That important distinction has researchers strongly recommending that young patients be referred for genetic testing. This can explain those special risks and create more appropriate treatment plans, and alert other family members as to special monitoring. Critically it may change the approach to any removal of the kidney and/or tumor.
Typically a small renal mass might be monitored or removed by either surgery or some laser ablation. If removed, the tumor can be assessed by a pathologist–a look under the microscope.Without a prior biopsy, the ablated tumor will not be examined, and no genetic testing can be done.
BIG HOWEVER HERE: even with a good pathology report, that may tell only what that tumor looks like–not what pushed it to grow, i.e., the genetic drivers. And those genes don’t go away with the tumor, so the risk remains that more tumors will grow, maybe in the second kidney, or in the partially removed kidney. Plus the rest that can happen with cancer…
An 75 year old whose small renal mass is removed will likely function well with one kidney. That same tumor in a 35 year old creates another challenge. If that tumor is driven by familial genes–not just by sheer bad luck–more tumors on the other kidney may be in the works. A partial nephrectomy must be considered. The risk of more tumors emerging in that kidney AND the other kidney is high. The younger patient needs decades of good kidney functioning, but those decades carry the risk of the emergence of more mets.
What else should trigger a genetic testing?
Quick answer: anything that doesn’t look like the senior citizen with a single tumor in one kidney. More officially below:
Early onset of kidney cancer is 46 years or less.
Bilateral (two-sided) or Multifocal (many locations) kidney tumors
Family history of kidney cancer, 1 or more close relative, 2 or more in more distant relatives
Kidney cancer with either a mix of other tumor types roughly related to kidney cancer or with lung cysts or pneumothorax (air leaking out of lung into chest cavity)
Personal or family history of kidney cancer syndromes.
The above list is from Yale School of Medicine, Professor Brian Shuch, who work includes dealing with heredity forms of kidney cancer.
More small renal masses found at an earlier age in more patients, as our imaging techniques improve and more CTs scans are done. Not all will be hereditary, and many will be sporadic or out-of-the-blue kidney cancers. Those are likely due to the sheer chance. Things go wrong as trillions of cells divide and make DNA mistakes along the way. Years of environmental damage may overwhelm the body’s ability to correct those DNA mistakes–i.e., the immune system gets overwhelmed, tricked, tired, etc.
Kidney cancer found at an early age or with the bilateral/multifocal tumors simply must be tested as to it genetic origins. This gives information critical to protect the rest of the kidney(s) and to participate in treatment that is more helpful. Finding an effective treatment will still be a challenge, but proper treatment requires knowing exactly which kidney cancer you have. From there, a real plan can be developed.
Just as I remind all readers to work with an experienced RCC oncologist–not just a surgeon and/or urologist (sorry guys, we need a team)–those who fall into this early and hereditary renal cell carcinoma category must also work with super specialists.
The person to contact at NIH is genetic counselor Lindsay Middelton at (301) 402-7911. She is with the National Cancer Institute’s Urologic Oncology Branch. An introductory link is below to the NCI and two other rare kidney cancer organizations.
In our kidney cancer world, it is unusual even to know the name of the radiologist, and most patients rely on his report, as given to the doctor. Many kidney cancers are “incidental findings” on CTs given with another diagnosis anticipated, broken rib, for example. Thus, it is the radiologist who recognizes the cancer long before either the doctor or patient. It may be a metastases that is found, with the primary tumor not yet imaged, or vice versa. If the tumor is relatively small, and no mets are seen in that initial scan, most patients are assumed to have localized disease. Often there are sudden plans for surgery, but not necessarily to search for other distant mets. The patient may be told, “I got it all.”
Of course, that is the best news, and the only news we want to hear. But we are wrong, as what we NEED to know, even before the surgery, is whether or not there has been a spread of the cancer. Treating kidney cancer is already a guessing game, and without knowing the whole game and all its rules, the patient is too often the loser. (Look for a longer, somewhat geeky post on small primary tumors and their potential to metastasize, both quickly and years later. Ain’t a pretty picture.)
Any good radiologist will know that even small primary tumors can have already produced distant mets. That radiologist likely knows that additional imaging should be done in such cases. The GP or even the urologist without RCC experience may NOT know that.
Too often small, overlooked mets in the lungs or on a bone can go unnoticed for months or years. Only the radiologist can provide a complete understanding of the extent of the cancer, and only with imaging outside the area of the “incidental finding”. He is the first line of defense, and often the first real expert in determining the extent of the disease. Thanks to those unsung heroes!
Is kidney cancer really so resistant to radiation? Many studies indicate that kidney cancer is far more resistant to radiation therapy than many other cancers. RCC just doesn’t behave as other cancers do, so the most knowledgeable doctors use radiation very carefully. The typical wider damage that comes with general radiation is not balanced by a good response in RCC. To be effective, a more specialized radiation is needed.
One of my most knowledge SmartPatients/friend has provided important information about radiation and RCC. The following is a link to videos, and is followed by advice to a fellow patient trying to understand her options. SBRT is Stereotactic Body Radiation Therapy, and not at all the same as general radiation, as is explained..
“For right now let me sort of define whats important about SBRT and why it works on RCC. SBRT is all about high daily dose needed for radioresistant cancers.
What is important is the high daily dose for RCC used in SBRT. For example, an SBRT plan for a lung met will use 3 fractions x 15 Gy/day or 5 fractions x 10 Gy/day. Fields will be very conformal to the tumor (but usually not by using shaped fields)
Forget shaped. Conformal small fields–yes.
An IMRT (Intensity-modulated radiation therapy) or shaped conventional plan might use 25 fractions x 10 Gy/day.
And to give daily doses of 15 Gy you need excellent imaging and mechanical capability that not every machine has.
Does it matter? Yes! The recurrence rate for RCC is much higher with low daily doses. The SBRT dose regimes will give about 90% local control (meaning that met never comes back-if you get cancer, it is a new spot.) Standard dose regimes give more like 60% long term local control.
SBRT typically uses dose modulation(which may or may not involve shaping beams ) to control where dose goes.
MLC or block shaped beam IMRT IMRT/IGRT-all use shaped beams but are not SBRT.
Cyberknife and Gammaknife, for example, use no beam shaping-they use hundreds of tiny identical circular pencil beams to build dose covering the tumor.
ANALOGY: Let’s say you have a huge thistle in your lawn. And you have a cup of Roundup. You can go outside 3 days in a row and put 1/3 of a cup on it. Or you can go out every other day for a month and put a spoonful on it. You are more likely to kill it for good with the first method. We want a quick thorough cell kill.”
This SmartPatient does not mince words. We all want a quick through cell kill, which may bring a met under control permanently. Not mentioned in this article, is that the body can also have an immune response in the area of the radiation, and deliver a burst of its own cancer-fighting proteins to the area. This can have an additional effect in countering those super-tiny mets that may be invisible, or just trying to establish themselves in the neighborhood.
Just as there are a range of antibiotics, and we know that the choice of each is dependent up the infection, its location, and the individual’s system, so it is with radiation therapy. Properly chosen, delivered correctly and to the exact place, with an understanding of the person’s disease, it may be a very effective tool to fight RCC, and not just clear cell.
I love this study, as it really symbolizes the tremendous change that has occurred in kidney cancer treatment these last 6 years. It is remarkable that the 124 patients are described as having already received first- line treatment, and were now in their second-line. These same metastatic patients might have received neither just six years ago.
The study was really not to compare the response to the treatments received, whether Sutent (sunitinib), Nexavar (sorafanib), or placebo. (Why any party chose or was chosen to receive a placebo is another, darker question.) That the median follow-up was 80 months is a triumph by itself. This is in contrast to the clinical trials that often show just a few months extra time which we and politicians can focus on, when the reality of much longer responses is clearly shown here. Of course, these longer survival times came from those trials which showed those few months–and this shows the reality of many more months and years of life!
Metastatic tumor burden(TB) was measured, based on the size of the sum of the longest unidimensional diameter of each targeted lesion. The additional increase of 1 cm (about 3/8”) was significant in predicting response to the medications. Siimply, adding the one-direction measure of the lesions and comparing them showed that more tumor was a bigger problem.
One can also assume that to remove as much tumor as possible may be helpful in maximizing the benefit of the meds given, although this study does not address the actual types and locations of the mets, nor indicate why no other therapies, surgery or ablation, were used. With 124 patients this would represent a mix of individual experiences, more like the typical patient group.
What does “median follow up of 80 months” really mean? A median is not an average, but a measure of the time point at which ½ of the population studied had follow up less than 80 months and ½ had follow up for more than 80 months. Since this is considered a long time in clinical trials and becomes more of a longitudinal study, we may never know the average length of time that these patients had either PFS (Progression Free Survival—time until the mets began to grow again) or OS (Overall Survival). In any case, we are aware that following this second-line of treatment, there are still more therapies and interventions which may be available. And even more options are up for FDA approval as I write.
All these options and the greater success of each muddies the study waters, but clarifies the hopes of those with metastatic RCC, or are at risk. This study proves that tumor burden (TB) is a disadvantage. Most patients have naturally assume that more cancer is worse for you than less cancer—who knew? But this gives weight to the notion that the removal of some tumors, if not all, can be beneficial used with targeted therapies. In the past, some oncologists have discouraged additional surgery in the light of metastases, with the implicit message, “It’s too late, and won’t help you anyway.” Not the doctor for me.
The story is quite different right now, but patients may need to tell this to their doctors–in the language that the doctor speaks. Certainly, there was a time at which doing more surgery for mRCC patients added little, if anything, to survival and probably even less to the quality of life. That no longer is the case, and those older studies no longer have meaning. While each patient must be treated as an individual, in light of all the variables that impact his health, there is increased optimism for the metastatic patient. Aggressive and early treatment can no doubt extend life and make it worth living.
The Small Incidental Renal Mass: Treatment Options
I have summarized and edited presentations from an April 2012 Kidney Cancer Association Patient Conference so patients can read and study them.
The original presentations can be found on YouTube offered by the KCA.
Poor resolution slides have been reconstructed
Treatment Options for the Small Incidental Renal Mass
After a brief welcome and expression of appreciation for the KCA, Dr. Karam begins:
“Currently, a small renal mass is defined as smaller than 3 or 4 cm, localized to the kidney, not invasive to other organs. This is a consensus and these definitions can change. Of all Stage I kidney tumors, 43 % are less than 3cm in size. (Some Stage I kidney cancers can be larger than 3cm; other treatments may be more suitable.)
I will discuss three options with patients who present with these types of lesions. The first is active surveillance, the least invasive, the next is energy ablation, and the third is surgical removal. Each will be discussed in the sequence.
First “Active Treatment Options” is energy ablation. This can be done through the skin, percutaneously, laporascopically, or be done “open”. Energy ablation includes two categories, Cryoablation (CA)–freezing the tumor, done laporascopically or through the skin. Alternatively is Radiofrequency Ablation (RFA), typically done percutaneously, or through the skin.
The second major category of active treatment is surgery, the standard of care being an open partial nephrectomy. That removes just the tumor, leaving most of the kidney. It is now more often being done as a robotically assisted partial nephrectomy. Another option is to do it laporascopically, with minimal incisions. Radical nephrectomy, complete removal of the kidney along with the tumor is the lowest on the list. It is the least favorable option, as we try to save the kidney, wherever possible.
AUA (American Urological Association) Guidelines have published some guidelines, based on multiple studies and experts. The standard of care for treatment of small kidney masses is partial nephrectomy. A radical nephrectomy is used only if the mass cannot be removed by partial nephrectomy. A recommendation could be ablation or active surveillance. This will be tailored to individual needs of the patient and the kidney, as to the location of the mass and its characteristics. No one recommendation fits all patients, and each must be discussed and individually tailored.
Next is active surveillance. We don’t use “watchful waiting”, but “Active Surveillance”. We do not to tell someone to go home with your small mass as we don’t need to do anything about it. On the contrary, we have to actively bring the patient to the clinic for CT scans.
What is active surveillance and what does it entail? That means doing no interventions, no surgery, and no procedures that are invasive–active surveillance. Initially we would do imaging at 3-6 months intervals in the first year, subsequently imaging at 6-12 months. There are no rigid guidelines at this point. I always tell my patients to be aware that we have only had small studies with active surveillance, and with short follow-up of 2-3 years. There is a very small potential for spread or metastases while we are doing active surveillance, so every patient has to be informed about all of this.
How often do small masses spread or metastasize? When does it seem to happen? This is a meta analysis of data from 18 studies with almost 900 patients. In only 18 patients of 880 did metastases occur while on active surveillance, a rate of about 2%. This spread occurred almost 3 ½ years after initiation of surveillance, so it does not occur in the first 3-6 months, more on average about 3 ½ years.
“How fast does a mass actually grow?” We know that 23% do not grow at all within 2 years or so. The rest do grow at the growth rate shown.Comparing the growth rate of those who had spread or metastases with those who had none, only 18 patients had spread. The group without spread was typically younger (66 versus 75), with a smaller mass at the initial presentation, 2cm versus 3 cm. The final size in centimeters of those who had spread, those 18 patients, was about 5.9cm. The tumor was quite large at the time when the metastases occurred, and here we started at a size of 3.1 cm.
The growth rate was about 2mm per year for the patients who did not have spread, and about 6mm per year for patients who did have spread. The time on active surveillance was about 2 ½ years.
Of these patients on active surveillance, what happened to them, did they all continue after active surveillance? Over half did remain on active surveillance, over a period of 2-3 years. Fewer than half had delayed intervention. They might have gone to ablation or surgery, and this is over a period of 2-3 years. Others had “delayed intervention, with patients having ablation or surgery on average about two years after starting active surveillance.
The common reason for moving from surveillance to intervention was typically patient concern about the growing mass—patient anxiety. The next reason was enlargement of the mass and the third one was that a patient had some bad medical problem initially not related to the mass. When that problem was solved, and became a good surgical candidate and they are switched to surgery.
Energy Ablation: Radiofrequency
Next is Energy Ablation, a more invasive category which includes radiofrequency and cryoablation.
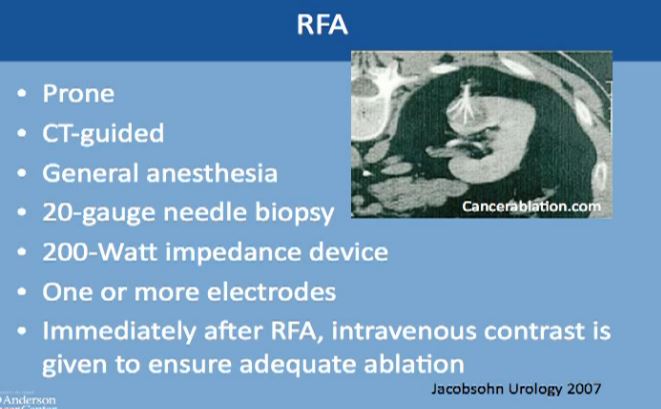
How does radio frequency ablation work? I usually tell my patients that is basically frying the tumors. The waves from radiofrequency cause friction and movement in the water molecules. This produces heat and destroys the tumor. Cell death occurs in about five minutes after exposure to the RF, with the temperature over 50 degrees Celsius )122 Fahrenheit. This can be monitored during the procedure. We have to achieve temperatures up to 100 (212 F)degrees in order to effectively destroy the tumor with this procedure.
This is a CT scan of the vertebral column and the patient is laying flat on this tummy. This is the kidney, this is the mass, and is CT guided. The interventional radiologist usually puts this thick needle with these tines, typically done under general anesthesia. Though we can do it very infrequently under conscious sedation, but general anesthesia is preferred. A biopsy is typically done at that time and one or more electrodes are inserted. Immediately after the procedure iss done, we do a CT to see that there isn’t any bleeding and to make sure this was treated adequately.
Energy Ablation: Cryolablation
(This is a video which can be seen on the Youtube video.)
The next category of energy ablation is cryoablation or freezing the tumor. This is a picture during laparascopic surgery. You can see them freezing the tumor. This is the kidney here, the tumor here. The tumor here has been marked; the electrodes that go into the tumor, freeze the tumor and form an ice ball.
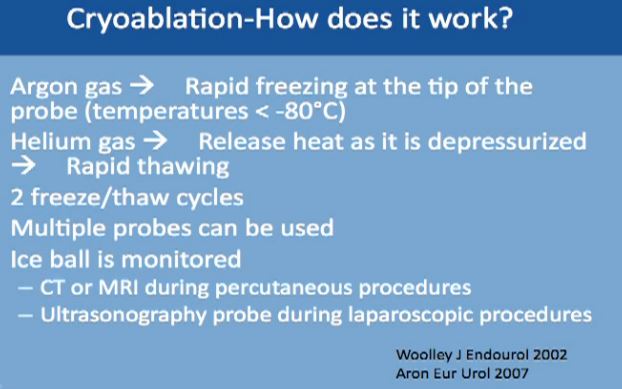
We use two gases for this procedure. The first is argon, which causes rapid freezing at the tip of the probes, with the temperature dropping to less than 80 degrees Celsius. The second gas is helium, which releases heat as it depressurizes, and it causes very fast thawing of the tumor. This typically repeated twice, two cycles of freezing and thawing. Multiple probes can be used to achieve tumor ablation. With this technique the ice ball can be monitored and you can see the progress with time. This can be monitored by CT or MRI, done percutaneously under guidance, or with an ultrasound when you are doing it laporascopically. or with an ultrasound when you are doing it laporascopically.
Cryoablation—How Does It work?
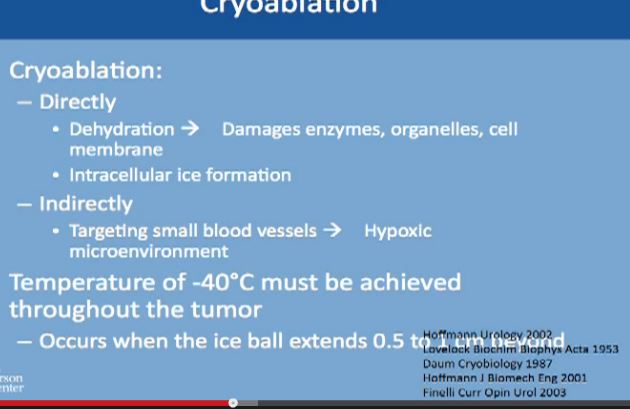
The Cyroablation acts directly on the tumor cells. It dehydrates the cancer cells, removes all the water from them, which causes damage to the enzymes which are needed for survival by the cells, the organelles and the cell membranes. It also causes the formation of ice inside the cell and kills the cell. But it can also act indirectly, as it targets the cells directly, cutting off nutrition needed for growth. In order to achieve this, very low temperature have to be reached, and to achieve it homogeneously for all of the tumor, the ice ball must extend ½ to 1 cm beyond the margin of tumor to make sure it is completely frozen.
Cryoablation
As to follow up, how do we know it is still working? There will be routine visits to the clinic with medical history, physical exams, chest imaging which is either with conventional radiography, CT and routine blood work.
Follow Up
To follow up on the tumor itself, we typically do a CT or MRI with IV contrast to visualize the tumor. The first follow up is at 6 weeks after the ablation to make sure the ablation was complete and successful and then at 6, 12, 18 and 24 months after ablation.
It does not mean that follow up will end at 24 months. The patient continues with scans for life, routinely, at least once a year after deletion or the treated tumor is stable. So imaging has to continue for years, as we don’t have long term studies with these technologies.
We tend to do more biopsies if the mass is not shrinking well enough, or if it is taking contrast, or it doesn’t look right one year. If the mass is not looking right, we go ahead and do the biopsy to make sure there isn’t any recurrence.
Recurrence defined after ablation can be tricky because the mass is still there. A successful ablation is defined as lack of enhancement of the tumor with the use of contrast. That is why is it very important for the patient to receive and tolerate contrast IV contrast for follow up after ablation. With cryoablation, typically you see tumors shrinking. With Radio Frequency, it doesn’t always happen. That is what makes it trickier, so we have to do biopsies for patients after treatment. And again, the tumor does not always shrink; more typically it does with the cryoablations. Again, radio frequency ablation lesions don’t always shrink, so absence of enhancement is what we look for which is not always ideal.
Now we always discuss with our patients the potential need for biopsy after ablation so this may be expected, though is not routine. Thus, the patient has to be aware of this. We don’t do it routinely, but it is a possibility.
What can predict who is going to have a successful ablation? Tumor size less than 3 or 4 cms is a very good indicator that we will be able to successfully ablate the tumor. If the tumor is exophytic, that the tumor is not deep into the kidney, this is a good indicator. If the tumor is peripheral or not central, that means that the tumor is away from the artery and the vein of the kidney. This is also a very good indicator that we can successfully treat it with ablation.
There are some complications, including pain after the procedure. This is usually an overnight stay; the patient goes home the next day. There could be some numbness or neuromuscular complications. There can be some air around the lung, if the needle had to be inserted close to the lung. This is typically monitored during the procedure.
Seeding from the tumor is exceedingly rare, maybe 1 or 2 cases, so exceedingly rare, nearly unheard of, so this should not be a concern for patients who are willing to go through this procedure. Bleeding can occur, and that‘s why we like to keep patients overnight. Also there could be some strictures or narrowing of the ureter tube that drains the kidney.
So how do we know to recommend RFA or Cryoablation?
We know RFA is considered easier, faster, and safer, but actually has a higher chance of doing damage to the collecting system, the system that drains urine from the kidney. On the other hand, CA has a slightly higher risk of bleeding compared to RF. But it is better for larger tumors, and is good for deep tumors or central tumors. You can monitor live CA with ultrasound or CT to see the ice ball actually grow and treat the whole tumor.
Partial Nephrectomy
The more invasive category is the partial nephrectomy, the actual removal of the tumor, leaving the rest of the kidney in place. The standard had been the open procedure, but nowadays, people tend to do more robotic assisted surgery. You have to have a good surgical candidate for this, both as to the patient’s anatomy and the actual mass. Less commonly used is the pure laparoscopic, just because it is technically challenging and because most hospitals have a robot available.
(VIDEO available on Youtube, about 17 minutes into clip.)
We will show a two minute clip of robotic nephrectomy surgery, courtesy of my colleague. The kidney is here, artery to the kidney here and the vein to the kidney is here. First we need to stop the blood flow to the kidney to do this procedure safely and accurately. A clamp is temporarily placed on the artery and another clamp on the vein, which will completely shut off the blood supply. Here the tumor is literally being carved out of the kidney. Here is the tumor, this is normal kidney, this is tumor, and this is the tumor over here, normal kidney here, so this is what is considered a partial nephrectomy. We check that the mass is excised and then suture the kidney so we can get normal control and prevent bleeding. All you see here is normal kidney. (This is on slightly fast forward–we don’t typically work this fast!)
So now they are bringing back the edges of the kidney together. We use some substance to prevent bleeding which will dissolve on their own: bringing the edges of the kidney back together. And you can see very early on that very little of the normal kidney is removed, just to give a margin to assure that we remove the whole tumor. We remove all the clamps to bring back normal blood supply to the kidney, so this is how the kidney looks. It is pink because it has the normal blood supply. There is no bleeding seen.
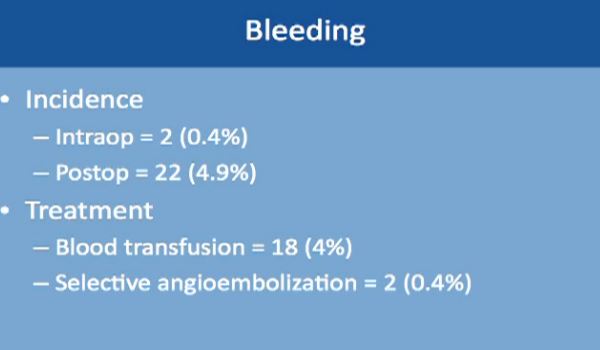
Complications might occur in some procedures. This is a large study of almost 500 robotic-assisted partial nephrectomies. Tumor sizes were about 3 cm, so small kidney masses. The total complication rate is about 16%. Complication rates include everything, even slight fevers, so higher than you would expect. Less than 2% of the complications happen during the surgery; most of the complications happen afterwards. About 99% of the surgeries were completed with a robot. Main complications specific to a robotic–assisted partial nephrectomy are bleeding, urinary leakage (1.7%), radical nephrectomy (1.6%), which means removing the whole kidney.
Bleeding occurred in two patients only during the operation, and about 5% of patients while they are still in the hospital. The treatment is relatively simple. Blood transfusion took care of 4% of these patients. About 2% of these patients needed selective embolization, a procedure that is usually done by interventional radiology and done under sedation. This saves the kidney and controls the bleeding as well.
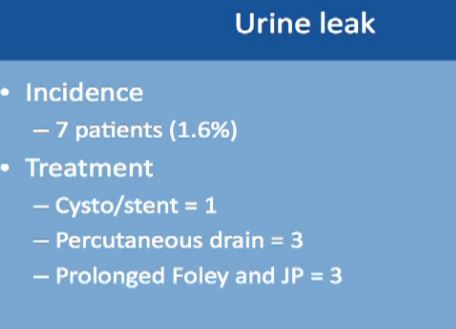
Urinary leakage is found in less than 2%, with treatment typically to put in a stent or a drain or leaving the catheter in longer. None of these patients needed repeat operations or removal of the kidney.
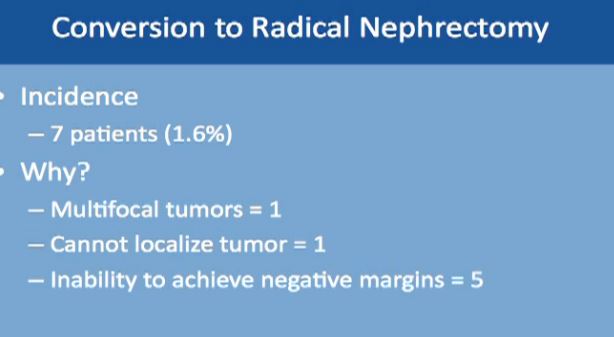
Another complication is conversion to a radical nephrectomy, which occurred in less than 1.6% of patients. This may be due to finding multiple tumors not recognized earlier. In one patient, the tumor could not be found; this happens if the tumor is small and very deep into the kidney. In five patients, a negative margin could not be achieved. That means some cancer was left behind after the tumor was carved out. Then the physician decided to remove the whole kidney to make sure all the cancer was gone. Also, one or more tumors cannot be removed successfully with the kidney left in place. Such complications occur less than 10% under any procedure.
In this table (which could not be captured), but the tumor size was about 3 cm on average. Surgery time was about 3 hours. Blood loss was about 200-300 ccs and hospital stay was about 3 days. This is a different study with complications about 5%. And with positive margins, i.e, a tiny amount of cancer was left, was about 1.6%. The follow up was about four years.
Complications after Treatment Now to compare the rate of complication with RF and cyroablations and surgery: this is from the AUA guidelines; the complication with Cryoablation is about 5%, with RFA about 6%, about 9% with lap partial, and about 6% with open partial and about 3% with complete removal laporascopically, and about 1% with open. All are less than 10% complications.
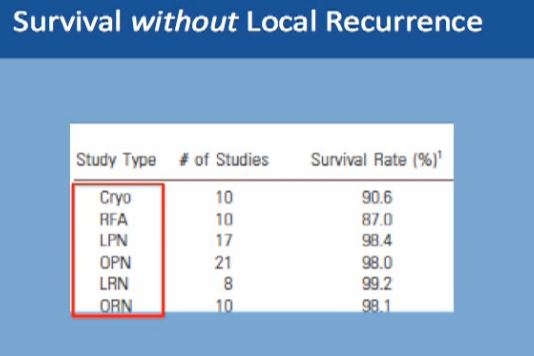
What about survival without a local recurrence?For cryoablation, it is 90% This is not complete survival, this is living without a recurrence. Again, 90% with cryolablation, with RFA about 87%, and with surgery about 98%.
Renal Function
Partial nephrectomy and RFA has similar renal functional outcomes
No change in GFR
No change in CKD stage
Kidney function is pretty much the same after these procedures, whether you do a partial removal of the tumor or an ablation, so that is not a major factor in decisions.
Active surveillance should be offered to appropriate patients. Patients should be informed that metastases could happen, but typically less than 2% of the time, and it typically takes on average 3-4 years on average. before that would happen. Half of all patients will undergo some treatment eventually, and leave active surveillance.
Survival without Local Recurrence
With the second modality, energy ablation with radio frequency or cryoablation, the chances of survival without local recurrence are about 88-90%, and we have intermediate term data, but not long term follow up on those patients.
However, with surgery you have 98% chance of survival without having a local recurrence to that same kidney. With surgery, we do have long term data as to partial nephrectomy.
A partial nephrectomy is the most definitive therapy. Any patient who is willing to undergo surgery and can tolerate surgery should do have partial nephrectomy for small renal masses. Alternatively, we can offer patients surveillance or ablation. We typically reserve that for that for those with poor kidney function—and we don’t to cause more kidney dysfunction, for those with more have multiple tumors, or for the patient at a high surgical risk or with a poor performance status. That latter patient means he might be a poor surgical candidate due to other health issues, with a heart problem or more dangerous tumors, for example. We can offer surveillance or ablation for those patients. If patient does not want surgery, we can offer two other options. This concludes my talk and I welcome questions.”