Kidney Cancer Association National Patient Conference
Dr. Eric Jonasch; MD Anderson Cancer Center
April 14, 2012
Systemic Targeted Therapy for Metastatic Renal Cell Cancer in 2012
I am going to talk as systemic targeted therapy for Metastatic Renal Cell Cancer, what we are currently using andhow we are using it, and the science about it, and how that leads us to new ideas, moving forward. Although I can see people here benefiting from what we do it is not enough.
When we talk about kidney cancer, we cannot talk about just one disease type. What I am going to talk about mainly is clear cell, and Dr. Tannir, my friend and colleague, is going to talk about the non-clear cell subtypes.
So what is ccRCC? It is essentially a cancer that looks like this under a microscope, and it was called this, back in the day. We more recently found that it has a mutation in the VHL gene (Von Hippel Lindau) in the large majority of individuals with and I also run a clinic where I try to marry the information we have about hereditary kidney cancer with non-hereditary kidney cancer to improved therapies.
Slide 2: This is not to scale; it is 213 amino acids long and for the scientists in the audience, that is mercifully short, and it also has three exons in or three parts, or easier to study than most, but obviously still hard to study.
Slide 3:
What it does, it essentially regulates how the cell reacts to oxygen. Obviously oxygen is our life’s blood, we need oxygen to, we need water, we need glucose. And our cells, if they feel like they hve enough need oxygen, they basically sit back and VHL will then take the transcription factor, it breaks it down If you have low oxygen state, then the cell will say, “Help, I need oxygen” and the VHL will step back, the transcription factors, HIF alpha and HIF beta are going to come together and you will get production of proteins, like VEGF which is a growth factor for blood vessels and some other things. If you have a mutation or something how an inactivation of the VHL gene, you have essentially this ongoing process of these cells, now cancerous, saying—somewhat untruthfully—we need more oxygen, we need more blood, build me an infrastructure.
Slide 4
That infrastructure is as follows: When we think of cancer we can’t think of cancer cells The cancer cells are in black on slide and in blue above, the stromal cells–the “glue” cells, and above those the endothelial cells or blood vessel cells. This triumvirate plus other cells generate an organ—and it really is an organ—that we call cancer. And when we use therapies, we are blocking specific areas there.
I’ll tell you a bit about the therapies we use now and that some of you are on, and what they are actually blocking.
Here is some terminology you are about to hear, some jargon, as we talk about trials and therapies. 1) Progression free survival (PFS)—time it takes for cancer to start growing again and 2) Overall Survival (OS)—time it takes from start of treatment to passing of patient
So the “blood vessel starving” are the five antiangiogentic therapies we currently have are listed here, and I am going to go through each of these in details.
We also have some up and coming drugs. And the way these drugs work (Slide 4 again) is by blocking the blood vessels. They try to kill the blood vessels that feed the cancer. They don’t seem to have much effect on the cancer itself. That is why you have experienced that we can shrink this down, but we can’t make it go away. And what we need, and on our wish list, are kidney cancer cell-killing therapies for the future.
mTOR FDA approved;
Temsirolimus (Torisel)
Everolimus (Afinitor)
The mTOR inhibitors, of which there are two, Torisel and Afinitor, Temsirolimus and Everolimus.
What they do; they are actually working inside the cell both perhaps in the cancer and blood vessel cell. And they are blocking particular proteins that seem to be up regulated, overexcited, in the cancer cell that give them a selective growth advantage.
There we have on the bottom, kind of a brown color, mTOR, which if it is overactivated, results in production of and more survival … for the cancer cells—which is shouldn’t have. What Torisel and Afinitor do is to block that signal.
So we could predict who was going to respond in the primary tumor, so the question was, “Can we use that as some sort of bio-marker?”
PART Two of Several Parts;
“Cytoreductive Surgery for Metastatic RCC: It’s Not for Everyone”
Dr. Christopher Wood
Integration of Surgery and Systemic Therapy in the Treatment of Kidney Cancer
Also referred to in the KCA program as “Role of Cytoreductive Surgery in the Treatment of Metastatic RCC
UT MD Anderson Cancer Center
April 14, 2012; KCA National Patient Conference
Cytoreductive Surgery for Metastatic RCC: It’s Not for Everyone
Identifying Patients Who Will Not Benefit from Cytoreductive Nephrectomy
Cytoreductive surgery is not for everyone. Certain patients will not benefit from surgery. We (MD Anderson) did a study to see if we could accurately select those patients who would not benefit from such a surgery, to save them from a surgery likely to be highly morbid and not beneficial. We compared 566 patients undergoing surgery to a group of 110 patients were treated with their tumors in place and treated with medical therapy only.
We tried to predict for which (patient) factors predicted outcome. We at MD Anderson can be very aggressive in our surgeries as we believe in cytoreductive surgery, so these patients who could not have surgery were probably the worst of the worst. For these patients, treated with medical therapy only, the median survival was only 8.5 months.
With that in mind, we looked at those patients who underwent surgery. If those patients did not live beyond 8.5 months after surgery, they probably did not benefit from that surgery. What factors predicted for those patients to live longer than the 8.5 months than did the medical therapy alone group?
What factors would be predictive of how one would do? We identified the above factors; low serum albumin, an overall nutritional status lab value, elevated LDH, also a blood test, the presence of liver mets, presence of symptoms due to those metastases, retroperitoneal lymph node involvement, (discussed earlier as a bad sign),supra-diaphragmatic lymph nodes and locally advanced T state. All of these features predicted for a worse outcome.
If a surgical patient had three or fewer of those features, he did significantly better than those who received medical therapy alone. But if a surgical patient had more than three of these features, that outcome was the same or worse than those who received medical therapy alone. So now we are using these features to prospectively select patients for surgery.
Can We Do Better?
Is the relevant question whether or not surgery should be incorporated into the management of metastatic kidney cancer?
I argue the more relevant question is whether there is a role for “pre-surgical therapy” for metastatic kidney cancer.
Pre-surgical therapy means to give some targeted therapy for some defined period of time, then go to surgery and resume targeted therapy after surgery. The potential benefit may be to use the pre-therapy as a selection process: patients who do well are those taken to surgery, and the ones not doing well are spared a surgery that not likely to give them benefit. It allows us to harvest (surgical) tissue that has been treated with these agents. With that available, we can study it to see how targeted therapy affects the tumor, what pathways are turned on and off, to help generate the next treatments. It may shrink the primary tumor and make the surgery easier, most important this is that it allows us to spare patients from surgery that they are not likely to benefit from.
However, targeted therapies don’t just target the tumor. They also target wound healing, which is why many patients who get this therapy have wound complications. The tumor will not respond to the therapy and may grow; a patient who was a surgical candidate all of a sudden becomes not a candidate for surgery, because the tumor has grown. He may need a more extensive surgery. The more I take out, the more difficult it is for you. And timing is everything. If you get targeted therapy and respond well, why stop that to send you to surgery? And as a surgeon, if you are not responding to targeted therapy, why would I want to take you to surgery?
Potential benefits are that the primary tumor may shrink, may downstage or downsize, and make surgery easier. Maybe we could do partial nephrectomies on everybody, save some kidneys. It may make the unresectable become resectable. It may improve prognosis. In patients without metastatic disease, it may eliminate micro-metastatic disease. (Pre-surgical targeted) therapy might be used as a litmus test of response, but there are risks, including surgical morbidity and lack of response. Plus there is pre-clinical data which suggests that in some cases, targeted therapy, treated in this fashion, may make the biology of the disease worse.
This is the MD Anderson trial with Bevacizumab (Avastin), where patients were treated with Bevacizumab for two courses of treatment and then went on to surgery and back on Bevacizumab after surgery.
We recently completed this Sunitinib trial. Patients completed two courses of Sunitinib, followed by nephrectomy and went on to receive Sunitinib post operatively when they had a response.
This is my Axitinib trial, where patients with locally advanced disease would receive three months of Axitinib, and go on to get a curative nephrectomy
Dr. Kamar showed you earlier an evolution in surgery over time. Ten years ago, everyone got an open nephrectomy; it was done open and very morbid. Then people began to use a partial nephrectomy and then a laparoscopic nephrectomy.
Each advance had to prove it was equivalent to the existing technique doing then and each had to show oncologic equipoise, i.e., equivalent cancer control. To give equivalent cancer control was the most important hurdle for each advance in order to be accepted. It also had to spare nephrons, for me, that the least important thing was this it was minimally invasive. Between a minimally invasive operation that doesn’t work, and a maximally invasive operation that does work, which one would you choose?
Similarly this neoadjuvant approach has hurdles. It must be safe and it must have improved outcomes. The least important is that it downsize or downstage the tumor. It is the rare patient who presents that you can’t resect. It would be nice if the tumor shrank, but that is the least important, I think.
Is NeoAdjuvant Therapy Safe?
Is neoadjuvant therapy safe? This patient (on the left) went on Sunitinib, had surgery and went on to get Sunitinib after surgery. What I did not know as the surgeon, that the patient started Sunitinib two weeks after surgery. And he had complete abdominal wall dehiscence (opening of the wound). That is his greater omentum sitting on his abdominal wall. The patient did not even realize that he had a problem and went to the MRI for his repeat staging study. He had no idea that he had a problem, so went he came to clinic and we saw that we went, “Oh, my God!”
Referencing another slide not shown here: On the right is a patient on the bevacizumab trial who had abdominal wall dehiscence, four months out from surgery. That is her small bowel (referencing upper portion of CT scan) and you can actually see it on the abdominal wall.
“Is this safe?” We did a retrospective study on 70 patients using pre-surgical therapy and compared them to 103 patients who had upfront cytoreductive surgery, and we looked at complications over 12 months.
Patients who had pre-surgery treatment did not have more complications than those who had upfront surgery, nor were there more severe complications. However, they were more likely to have late complications, and to have more than one complication if they had a complication. They were more likely to have wound complications, related to the targeted therapy and wound healing.
Looking at a multi-variate analysis, all the factors that predict for poor wound healing, the only factor that was significant was pre-surgical therapy.
Thus patients who get this therapy before surgery have a higher risk of wound complications—but not a higher risk of overall complications. They have a higher risk of wound complications, but for overall complications, it is the exact same risk as patients who got upfront surgery.
Patients who had a decline in their serum albumin while they were being treated had greater problems with wound complications. Serum albumin is seen as a marker for nutritional status. Now we follow that variable and find that for patients who have serum albumin decline, we are more likely to reinforce their wounds with surgery.
Happily, patients who received pre-surgical therapy did not have a worse survival than those who had upfront surgery, followed by systemic therapy. They may not do better, but they do not do worse, and that is an important feature and shown here graphically.
So What About Tumor Downstaging/Downsizing?
In the era of classical immunotherapy with interferon and IL2, with the primary tumor in place, the primary tumor never responded. That in part, was the impetus to take us to cytoreductive tumor, since the primary never responded.
These patients were treated here at MD Anderson. This is a patient had a very locally advanced tumor, and very large lymph nodes. Had this been done as cytoreductive upfront surgery, it would be a huge operation. Treated with Sunitinib and he had dramatic regression in the primary tumor, the nodes all went away, and he was able to have a laparoscopic nephrectomy. Arguably, he benefited from this approach.
This patient was treated with Axitinib for a very large locally advanced primary tumor here, treated with Axitinib, (on right CT). On the right, there was dramatic regression of the tumor.
Here’s a look at the specimen we removed. Here is the tumor sitting in the kidney right here, and arguably, this patient could have been treated with a partial nephrectomy. We wanted to do that, but they were reluctant.
This is another patient treated with Axitinib, that received neoadjuvant therapy, and again you can see (on left) a very large locally advanced tumor sitting in the right kidney. He received Axitinib and after three months, and you see a dramatic regression (right CT). With this he would have had to receive an open nephrectomy and with this, this patient can undergo a laporascopic nephrectomy. Much less morbid.
Here’s a picture of the specimen, dramatic improvement. All of this used to be viable tumor, nowhas been killed by the Axitinib and this rim is the tumor present.
Are These Just Anecdotes, or Can We Rely on These Agents to Downstage Tumors?
I would argue that if it is true, as a surgeon, I would say, give it to everybody. Maybe we can offer partial nephrectomies to all our patients.
S
So what is the data? This study looked at 17 patients treated with their primary tumor in place with Sunitinib. Only 23% of the patients actually demonstrated had a response, but those that did had a response rate of 31%.
At the Cleveland Clinic, the patients were treated with Sunitinib, and the overwhelming majority had little or no response in their primary tumor. In some patients, their tumor grew while on treatment.
Data from our Bevacizumab trial shows the recurrent theme; the overwhelming majority of patients had little or no response in their primary tumor to targeted therapy.
The University of North Carolina tested Sorafenib. Again, there were some dramatic regressions, there were some dramatic progressions, but the vast majority of patients had little or no response in their primary tumor.
Trying to determine once and for all, we want to ask whether there should be this treatment with the tumor in place.
In a larger study of 168 patients treated with tumor in place, we looked to see there would be tumor shrinkage.
Reasons for not removing the tumor is below, with the vast majority not considered good candidates for surgery, or were enrolled in a clinical trial.
These were the therapies they received. The vast majority received Sunitinib, which is the frontline standard of care, with other therapies intermingled.
As to the response rates, we had some patients who had dramatic progression of their tumor, some patients who had dramatic regression of their tumor. The vast majority of the patients had little or no response in their primary tumor.
One of the things that is common in the community is that patients with large venous tumor thrombi may hear their community oncologist say, “Here, take this medication, it will shrink your thrombus and it will make your surgery easier.” So is this data true?
A significant patients will present to me on Sunitinib. In this series, 48 patients had different levels of tumor thrombi and were treated with these agents.
Unfortunately, a recurrent theme (references “Stable Disease in 75%), patients had little or no response in their tumor thrombus. In fact, 15% of patients progressed while in treatment. Only 10% of patients demonstrated shrinkage in their venous thrombus in response to treatment.
Initial Body of Evidence Would Suggest that Significant Primary Tumor Downstaging Will NOT Be Realized with the Current Generation of Targeted Therapy Agents
I would suggest that the initial body of evidence suggests that significant primary tumor downstaging will not be realized with the current generation of targeted therapy. Nevertheless I must confess that I have been quite impressed with the responses that we have been seeing with Axitinib. Every patient has had a response.
As to the report card on presurgical/neoadjuvant therapy. I would argue that it is indeed safe. We see more wound complications, but those are pretty easily dealt with. It does not seem to reliably downsize tumors. I would this does not. Is this worth doing? Should we continue to do this clinical research at MD Anderson and around the world to determine if neoadjuvant therapy has a role in the treatment of patients? I would argue that it does for the following reasons.
In our Bevacizumab trial, 50 patients were enrolled, but only 42 underwent nephrectomy. Six patients had disease progression and went on to salvage systemic therapy rather than nephrectomy. These six patients were saved from a surgery that would not benefit them.
In our series, we asked, “Is there something about pre-surgical therapy that we can use to predict prognosis, and can we use the primary tumor as a bio-marker to predict outcome?”
This is a spidergram looking at primary response in the tumor. We noted is that patients, who did respond in their primary tumor, they responded early. If you don’t see it early, you will not see it; there is no sense to continue treatment if you don’t see some shrinkage.
Those patients who had at least a 10% reduction (in the first 60 days) in their primary tumor size went on to have their tumor shrink almost 25%. If patients did not have that 10% in the first 60 days, they were likely to have little, if any response.
So we could predict who was going to respond in the primary tumor, so the question was, “Can we use that as some sort of bio-marker?”
We treated 75 patients with Sunitinib with their primary tumor in place, and we found that those patients who had a greater than 10% response in their primary tumor had a significantly greater survival than those patients who did not have that early shrinkage of greater than 10%. If they had a greater than 10% response within 60 days, their survival was even better.
And that was in univariable analysis, and it also held up in multivariable analysis.
For the first time, looking at the primary tumor’s response to targeted therapy could be used as a prognostic variable for outcome of patients.
In Europe, there was another study, looking at Sunitinib. They arrived independently at the same conclusion that we did, that those patients (treated with their primary tumor in place) with a greater than 10% response in their primary tumor, when treated with their primary in place, had a significantly better outcome than those treated patients who did not.
Cytoreductive Nephrectomy for Metastatic RCC in The Era of Targeted Therapy
Not a question of “IF” but “WHEN”?
I argue that cytoreductive nephrectomy is not a question of “if”, but really more a question of “When?”
58
This trial that is currently ongoing in Europe through the ERTC, the CERTIME trial. Patients are randomized to cytoreductive nephrectomy followed by Sunitinib versus two course of Sunitinib followed by nephrectomy. This examines timing of the nephrectomy, not whether we should be doing a nephrectomy. This is a much more relevant research question, and this trial is accruing quite nicely over there.
In conclusion, targeted therapy has dramatically improved the outcomes for patients with metastatic RCC. Efficacy in the adjuvant and neoadjuvant setting still is under investigation. Without complete responses from this targeted therapy, surgery will remain an integral part of a multi-disciplinary approach, both as to control of the primary tumor and as metastasectomy. Show me an agent that demonstrates reliable and complete response, I will be the first to argue that we need to reexamine the paradigm.
Do not think that pre-surgical therapy is the standard of care. It is not. It has merit, but it needs further study and validation. It is not clear to me when it is appropriate to integrate surgery into the context of receiving systemic therapy. Thank you very much for your attention.
END OF LECTURE>
Questions and responses from audience.
Audience. “My question is regard to your last comment, as to the immediate impact of say, Sutent, showing up prior to surgery with an early response, does that also mean that Sutent–having a response in metastatic disease–does that tell you than an early response also means a generally better outcome?
Dr. Wood: I’ve got to tell you we haven’t looked at that, but that is a very worthwhile study to do. Intuitively, my answer would be yes, but I don’t think that we have anyone who has done a formal study on that. It is a very good question.
Audience: “How should ablation and the small tumors be monitored if you have those small tumors like less than 3 cm, like if you are a tumor producer, if you have “multi-foci” tumors?”
Dr. Kamar: Do you mean after or before the ablation?
Audience: “Before the ablation.”
Dr. Kamar: While you are on active surveillance?
Audience: “Yes, and if you have multiple primary tumors less than 3 cm.”
Dr. Kamar: This is more common in patients who have VHL syndrome, which is a syndrome where patients have a tendency to have more than one tumor in their kidneys. The follow up is every six months or so, so we don’t really want to image too often for the radiation risks that are involved with doing too many CT scans. Initially every 3-6 months and after the first year, move to every six months or one year. It also depends on whether the patient is young and healthy and why would we want to observe. In VHL patients that is done commonly, because we wait for the tumors to become 3 centimeters before we intervene. We don’t want to do surgery when the tumors are only 1-2cm in that particular patient population.
Wood; The 3cm we are talking about comes from the NCI where they have a huge experience in treating genetic kidney cancer, and they noted that patients with tumors 3cm or less never metastasize. So we use that 3cm size as a sort of trigger to tell us when we need to do surgery. With multi-foci disease, once it hits that 3 cm size, we will go in and debulk the tumors from the kidney, take all the tumors we can take out, and then follow them over time.
Audience: “I have a question re ablation. Is that an option if you have metastasized to your lungs?”
Dr. Kamar: You mean to use it on the lung tumor? (Yes) Do you mean on the mets or do you mean on the tumor in the kidney.
Audience: “No, my kidney is gone, but I have metastasized to the lung, and I have had cyberknife, but is it an option to be used on the lungs.”
Dr. Kamar: I think it is an option, but typically, if it is doable by surgery, which is the preferred way. The ablations that are done outside the kidney are mostly done for bone lesions, where cyroablation of RFA is done, because it is typically harder to remove a lesion from the bone than it is from the lung, for example. It is more commonly done for liver metastases if anything
Wood: It is more common to use it to treat symptomatic metastases, but there is some interesting work going on here at MD Anderson by one of our colleagues, where there may be some immunologic phenomena associated with ablation. We have some case studies that have been done, where patients who have undergone ablation, particularly RFA, not so much Cryo and had a complete regression of their metastatic disease, almost like a vaccine had been put on the met, and actually Seren is studying that with alone and with some of the immunologic agents that you will hear about from Dr. McDermott to see if that may be a viable treatment option for patients with kidney cancer in the future.
Audience: “After ablation, do you usually see necrosis in the body of the tumor? Can you see that during imaging?”
Kamar: You can see that afterwards, and typically more common with cyro. You see necrosis, coagulative necrosis. Typically it is coagulative to the tumor. You see that on the pathology, when you end up removing that tumor later on. So what we see is absence of contrast enhancement. The tumor before treatment was lighting up when you give contrast. After the procedure, it stays dark. That is our best indicator, other than biopsy, that the tumor is really treated by radio frequency. We don’t see really necrosis on imaging quite like for larger tumors like Dr. Woods showed earlier.
Audience: “So during subsequent imaging, you might see necrosis?”
Kamar: You might but typically what we look for is absence of enhancement. Necrosis is not something we reliably see or depend upon for follow up.
Audience: “For Dr. Wood, re venous thrombosis, do you insert an IVC filter prior to surgery, I’ve heard, or do you consult with cardiology to get that done. Is that helpful?”
Wood: Definitely that is not helpful before surgery. We have both had patients where some guy on the outside decided it would be helpful to put a filter in the vena cava, just in case a piece of the tumor thrombi broke off. It made surgery extremely, much more difficult. After the thrombus has been removed, in some patients we will leave a vena cava filter, which is like a screen put in the vena cave, so that blood clots below that screen blocks them from going to the lungs. A large pulmonary embolism could be fatal. So patients who do have evidence of a clot down in their legs, we will put a filter in, but if they don’t have any evidence of that, typically we don’t.
Integration of Surgery and Systemic Therapy in the Treatment of Kidney Cancer
Also referred to by the KCA as “Role of Cytoreductive Surgery in the Treatment of Metastatic RCC
UT MD Anderson Cancer Center
KCA National Patient Conference: April 14, 2012
The topic “Integration of Surgery and Systemic Therapy in the Treatment of Kidney Cancer” is near to my heart and in active research at MD A
nderson Cancer Center. The vast majority of patients present to us with locally advanced disease, and the reality is that almost half of patients with kidney cancer will at some time develop metastatic disease, which we all know is currently not curable.
Again, as to stage, the vast majority of patients present to us with locally advanced disease, and the reality is that almost half of patients with kidney cancer will at some time develop metastatic disease, which we all know is currently not curable. (Editor’s note: my stage IV RCC with innumerable lung mets in 2004 is now in remission or “cured”, or close enough to “cured”, that I must add this note. It is still shocking to understand that Stage IV RCC is considered incurable. PZ)
Six years ago, we did not have much to talk about. I could show this slide and sit down. For locally advanced disease, we took out the kidney; for stage IV disease, we took out the kidney and gave systemic treatment, usually cytokines.
Now we almost have too many therapies and don’t know how to use them all. How do we integrate surgery into the context of these treatments that we offer patients with metastatic disease? The sad reailties of this are no home runs. These therapies control the disease for some time in these molecular pathways they target. But in most patients, resistance will develop and they have to move on to the next treatment.
I will talk about how we integrate surgery into systemic treatment in 2012, the role of cytoreductive surgery, and then introduce the idea of pre-surgical therapy, something that we have been studying here at MD Anderson that has shown some promise.
These are two randomized trials, one in the US, the other in Europe, which demonstrate the benefit of patients undergoing cytoreductive surgery. The first is the EORTC trial where patients were randomized to upfront surgery followed by interferon, or by interferon alone.
Next is the SWOG (South West Oncology Group) trial done in the US, again demonstrating the value of undergoing a nephrectomy prior to interferon, versus interferon alone? Frankly, many surgeons referred to this trial as “Surgery followed by ineffective therapy is better than ineffective therapy alone.” You can see by these that the response was only 3-4%.
Now that we have more effective therapy, what is the role of surgery in the context of patients with metastatic disease? We don’t even know why cytoreductive surgery works. Does it just reduce tumor burden? Does it produce some sort of immunologic phenomenon where tumor antigens are exposed or is there an immunological “sink”. Is it an alteration in the metabolic milieu where taking out someone’s kidney and altering the ph in the body somehow is anti-tumoral? Or is taking out the “mother ship”, where some sort of endocrine or paracrine phenomenon that promotes metastases. We have absolutely no idea how it works.
Why not take out everybody’s kidney in the setting of metastatic disease?
The morbidity and side effects can be significant, and people can die from this operation. Though it has been proven beneficial in the context of interferon, and it’s quite possible that patients will spend the majority of their time left on earth recovering from surgery. We’ve seen metastatic disease explode post-operatively. Those patients never even get to go on to targeted therapy after surgery. Perhaps these new therapies will cause the primary tumor to shrink. Maybe we don’t need to take out everyone’s kidneys in the face of metastatic disease.
The French are testing this in their Carmena trial. Patients are randomized to an upfront nephrectomy followed by Sunitinib versus Sunitinib alone. It is a non inferiority study design, and the randomization is 576 patients. There is a problem; the trial is not at all accruing very well. Patients don’t like to have surgery randomized, with a computer saying, “You’re going to have surgery, and you are not”.
With the slow accrual to this trial it will be many years before we have an answer. Sunitinib may not even be relevant at that time. And what are we doing for patients in the meantime? Should I take the kidney out or not?
There is evidence that removing the kidney in the presence of metastatic disease is beneficial, from retrospective data derived from the expanded access trial with Sunitinib. These patients had their
kidney removed, not just cytoreductive surgery, but any time in their past.
They were compared to patients treated with their kidney in place. Patients who had their tumor out had a much better response rate than those treated with their tumors in place.
They also had a better progression free survival (PFS) and a better overall survival (OS) than patients treated with their primary tumors in place. Now this is retrospective, it is biased as it is not clear why the kidney was left in place for any one patient. That might have been because the patient was on death’s door and could not have had the kidney removed. But the data shows a benefit of being treated without having your kidney in place.
Newer data from Dr Toni Chouieri at Dana Farber compares are patients who presented with their primary tumors in place. Those who had the kidney removed prior to targeted therapy had a (overall) survival more than doubled compared to those treated with the primary tumor in place.
Those retrospective and (with patient selection) bias, it gives some guidance there may be some benefit to the removal of the kidney in the setting of targeted therapy.
Lecture continues as PART 2 with topic:
Cytoreductive Surgery for Metastatic RCC: It’s Not for Everyone
(The lecture is from a patient conference, and may be seen by clicking through to YouTube. My transcription may make it easier to STUDY the information from Dr. McDermott and to review the slides.)
Dr. David McDermott; Dana Farber Harvard Cancer Center; KCA Conference
April 14, 2012; MD Anderson Cancer Center; Houston, TX
“This is a great opportunity to talk about this new research. The last six years brought great advances to the treatment of metastatic kidney cancer with newly approved therapies. No other area of cancer that has had made more progress with new treatments in that time, and there is more good news to come.
In this era of targeted therapies, some have asked if immunotherapy–once the only option for kidney cancer–has any role. In the next twenty minutes, I will show you that it probably still does–for the proper patient.
Dr. Wood talked about limitations with the targeted therapies, the anti-angiogenesis drugs. They are excellent at pruning the tumor, much like I do with my weed whacker. Though they can delay progression, and improve survival, you need to be on treatment to have its effect and all these tumors come back. Once you are off treatment, the effect wears off. They can delay progression, extend life and patients are living longer.
There has been a greater understanding about how the immune system works over the last 20 years when this was introduced.
The Immune System
Adaptive defense system that protects an individual from invading microorganisms
The immune system is specific
Involves multiple large polypeptides that function in:
Antigen presentation
Antigen recognition
Intercellular signaling
Involves multiple cell types Slide 2
These insights can improve outcome for our patients. The immune system is a defense system, which protects the person from invading bacteria and viruses. This system contains multiple moving parts and multiple cell types.
Here is a cartoon example of all the different cells and antibodies, which can protect against bacteria, others that can target a microorganism, or more importantly, a tumor cell. This system was not designed to fight cancer; it was designed to fight infection. That means it is designed to turn on when you have an infection like a virus, and when the virus is controlled, the same “turned on” cells of the immune system are then shut off. These shutoff mechanisms are in part responsible why cancer can evade the immune system, and why it has been so difficult to use the immune system to fight the cancer, as opposed to fight infections.
Different approaches are being used with the immune system to fight cancer, some we’ve used in the past and some exciting new approaches currently being tested. The first approach is much like pressing on the gas. This approach to immune therapy has mostly involved cytokines, with interleukin 2 and interferon, and was used for a long time. They rev up the immune system and are growth factors that stimulate a lot of the parts of the immune system, such as T-cells.
Dr. Wood said there were no home runs for patients for Stage IV kidney cancer, but that is not exactly true. There are very few home runs, a few patients with stage IV disease who obtain a remission of their disease. Remission means treatment of Stage IV disease in which the cancer goes away, treatment stops, and cancer does not come back. To most patients, that is their goal. Very few patients meet that goal, but for some that remission has lasted decades.
Pressing on the Gas of the Immune System
It is also true that this “pressing on the gas of the immune system” does not work for most patients. It is hard to identify which patients it will work for and is associated with lots of side effects. To be effective, as with interleukin 2, these treatments must be given in a hospital. They involve serious side effects, sometime life-threatening side effects, so the kind of patient who can receive this type of treatment is relatively limited.
At Beth Israel Deaconess in Boston we try to be selective choosing patients for this therapy. We try to identify the patients who may receive the home run, before we put them through the side effects, because so many patients go through the side effects without benefit.
High-Dose Aldesleukin “Select” Trial in Patients with Metastatic RCC
D. McDermott, M Ghebremichael, S Signoretti, K Margolin, J Clark, JSosman, J Dutcher,M French, and M Aktins on behalf of the Cytokine Working Group
We had clues about things that might improve the selection, so created the IL2 SELECT trial, reported at ASCO two years ago. The activity of IL2 in this era of these new treatments is still relatively good, as good as it was 20 years ago. The response rate in this trial with 120 patients was 25%, significantly greater than it was when the drug was introduced 20 years ago. The drug is not any better, or are we any better at giving it. But we are better choosing our patients. Choosing who should get it, and who shouldn’t, and that improves the responses of our patients.
It has been known that patients with non-clear cell are less likely to respond to immunotherapy, so in this trial there were very few patients with non-clear cell cancer—and no responders in that group. It is also known that patients who had their primary tumor removed when they presented at Stage IV disease are more likely to respond to immune therapy. In this trial, 99% of patients had that surgery before they went into this trial. It is almost certainly true, that with new therapies available, that the types of patients being referred to an IL2 centers like ours is probably different. Changing the types of folks we are treat means our numbers are improving somewhat.
To improve the selection process and based on earlier research, we wanted to show that certain features of the patient’s pathology of the tumor might predict for response. We looked at what the tumor under the microscope and special proteins (CA IX or carbonic anhydrase IX) that the tumor might produce. We thought those things might predict either high chance for response or low chance for responding to treatment.
Unfortunately for me as a researcher, although fortunately for the patients who went on this trial, the folks who were in the poor risk group–those we thought would not benefit from IL2–did just as well as those not in the poor risk group. It surprised us and showed the importance of testing theories in the proper trials. We clearly need to do more work in this direction to find something to explain why some people benefit and some do not. And it may turn out that response may have more to do with the patient’s immune system than the cancer as how they benefit from treatments that boost the immune response to cancer.
RCC IL-2 SELECT Trial; Conclusions
Tumor features did not predict for response.
Efforts to confirm other predictors are ongoing.
Lessons from this work may guide the development of targeted immunotherapies in mRCC(e.g. CTLA-4, PD-1 antibodies) Slide 9a
So in conclusion for this trial, the tumor features did not predict for response, but we had a higher response than we expected higher than 20 years ago. This work continues and some of this work will educate us as we go into this new world of targeted immune therapy for kidney cancer.
So as discussed, the immune system is not designed to fight cancer, but to fight infections. This graphic shows where the immune system turns on in response, and at its greatest, starts to shut off, as it is designed to do. The shut-off valves of the immune system–the brakes–are in some ways stronger than the gas pedal.
Releasing the Brakes
In the laboratory over the past ten years we have been able to identify what are those brakes are. Now we ask how to block those brakes. One of the most important brakes on the immune system is a protein called CTLA-4 (CytotoxicT-Lykmphoctye Antigen 4). We can block the action of this protein, to release one of the most important brakes to immune response to cancer.
On this slide you see the T-cell on the left, an activated T cell, as it activates a protein, turns itself on. The same T–cell that turns itself on, puts out a protein on its surface, called CTLA-4. When that CTLA-4 protein comes in contact with another protein on that cell, an antigen-presenting cell, it actually shuts off the cell, a natural way of shutting off the immune response. That way these cells don’t overreact to an infection and attack healthy tissues, Now we can interrupt that interaction by bringing in a monoclonal antibody, which interrupts the connection between CTLA-4 and important proteins of the immune system. So we can block the natural shutoff that many patients experience.
Does that work to clinical effect with kidney cancer patients? The short answer is it does. Data presented in the New England Journal of Medicine two years ago. Blocking this protein in melanoma gave improved outcomes, and this was an out-patient treatment, intravenous, given every three weeks for four doses. It’s actually been shown to improve survival for patients with metastatic melanoma.
Blocking CTLA-4
And it’s not treating the cancer; it’s treating the patient’s immune system. The immune system is going out and detecting the cancer in ways that it might not have before getting this antibody. It is outpatient therapy, but it is still associated with significant side effects. Most of those are auto-immune side effects, where the body is now being attacked by its own immune system. Some of these are been quite serious and patients have died from this treatment. We are getting smarter at managing the side effects so there are fewer major complications, but do not get the impression that it’s not serious treatment. It’s less toxic than IL2, can be given to more patients, but still has side effects.
Ipilimumab in mRCC
Single institution (NCI), Phase II trial
Major response rate of 9%.
Max dose test 3/mg/kg. (Dose response in melanoma)
Survival effect in melanoma despite low response rate.
Additional studies alone and in combination warranted. Slide 14
This data led to FDA approval last year of Ipilumimab, now called Yervoy. It was approved in melanoma, but it has been tried in kidney cancer patients at the National Cancer Institute in a very small 36 patients, phase II trial. The response rate, the chance that the tumor shrank by half, was only 9% in this trial. That may not sound great, it was tested at a dose which may not be the right dose; higher doses of treatment may be tested in the future. In melanoma we saw improvements in survival and saw lasting remissions for Stage IV patients. We saw those benefits even with a very small response rate. Go to the “Blocking CTLA-4” slide, and look way out on the survival curve towards the end. These are patients out 3 and 4 years, still in remission and off treatment. That happened even though the response rate to treatment wasn’t very high. It is possible that we might see a long-term benefit for some patients with kidney cancer with an agent like this. Some others are being tested in the coming year, so I would be thinking that additional studies with this approach are certainly warranted.
Steering the Body’s Immune System
We need not just the “accelerator” and the “brakes” to make these things work. We also need improved steering. Investigators want to improve steering by giving patients vaccine approaches. This may get patients’ immune systems to recognize proteins found on the tumor, to wake up and to go and attack those proteins, and to try to control the cancer. These approaches are now in phase III trials that have shown some encouraging results, where we will get some answers.
The agent AGS-003 is being combined with the most commonly used drug for kidney cancer, Sutent. Patients are randomized to use either Sutent alone or Sutent with this drug. Whether this will lead to more response rates and to more long term benefit than with Sutent alone remains to be seen. At least we will get an answer from a large Phase III trial. One of the problems with immunotherapy trials over the years is that they haven’t been large enough to give us clear answers. But this trial is enrolling patients and there are others like it.
Putting up the Barbed Wire Defense
Since we’re in Texas, so I thought I’d give you a barbed wire analogy. One way in which tumor cells evade detection by the immune system putting up this “barbed wire” on their surfaces. When a T-cell comes, tries to sniff out the cancer cell, it is shut down, as opposed to going on to kill the tumor cell. We now know a little bit about that natural barbed wire which comes into play with this particularly important protein interaction, the programmed death pathway, and what that stands for is the inactivation, or the programmed death of the T-cell, which acts like barbed wire.
Why is this important? In kidney cancer, many patients’ tumors are coated with this barbed wire. Patients who have this on their initial tumor specimen have been shown to be more likely to have more disease recurrence in the future. Since we can identify the barbed wire, can we block its activity and lead to an improved effect? The question is, can we target this protein and can we improve outcomes? There is early evidence that maybe we can. This is a Phase I trial, admittedly very early.
Programmed Death (PD)-1/PD-L1 Pathway: The Basics
Several tumor types, including RCC, have been shown to over express inducible PD-L1
Over expression of PD-L1 by RCC tumors has been shown to be associated with adverse clinical/pathologic features, including the following:
More aggressive disease
Shorter survival
Also report to impair tumor immunity
Can PD-1 pathway blockage head to clinical benefit? Slide 18
Phase I Study to Evaluate the Safety and Antitumor Activity of Biweekly BMS-936558 (Anti-PD-1, MDX-1106/ONO-4538) in Patients with
Renal Cell Carcinoma and Other Advanced Refractory Malignancies.
Patients received an outpatient treatment, intravenously, with a drug that doesn’t even have a name yet, BMS-936558, a PD-1 anti-body. This is blocking the interaction between the barbed wire and T-cells. In this trial it is given every two weeks; on other trials it’s been given every three weeks. Patients were allowed to stay on this drug for up to two years as long as they were getting some clinical benefit.
SAFETY RESULTS; ALL PATIENTS
For the entire group, MTD (Maximum toxic dose) was not reached at doses of 1, 3, and 10 mg/kg
There was no apparent relationship between drug dose & AE (adverse effects) frequency
One treatment-related death
Grade 4 drug-related pneumonitis Slide 20
The main reason to do a phase I trial is to test the safety of the drug. This drug was found to be relatively safe, and we got up to the highest dose without getting into serious side effects. There didn’t seem to be a relationship between the dose and the side effects, which was good. There were still 10-15% patients who had serious side effects. In this group of kidney cancer patients and there was one treatment-related death, due to an inflammation in the lung that was probably contributed to by the drug.
SAFETY RESULTS; ALL PATIENTS
Any grade, drug-related (investigator attributed*) serious AEs (SAEs) occurring at a frequency >1% in the entire study group (n=126)
Total with an SAE=11%
Investigations=3.2%
Endocrine disorders=2.4%
General disorders and administration site conditions=1.6%
Hepatobiliary disorder=1.6%
Neoplasms benign, malignant and unspecified=1.6%
Respiratory, thoracic and mediastinal disorders=1.6% Slide 20a
This trial of 126 patients was a much larger group and not just a kidney cancer trial with five cancer types in this trial. There are now 300 patients in this trial, and we’ll get more data in the next several months. But in general the safety population is much larger than the efficacy population. The main point here is that serious adverse events occur in about 11% of all patients, much less than in HD IL2 and CTLA-4.
What did we see in terms of effectiveness? For the first 16 patients analyzed, we saw five partial responses (31.3%), and three patients (18.8%) with stability that lasted over six months. About 50 % of patients were getting some clinical benefit with this antibody. Once again, a small number of patients tested.
Here is an example of the patients we studied, a young man who was diagnosed in 2009, received IL2 and progressed, received Sutent and progressed, had disease in multiple places, including the kidney and the bones and lungs. You can see the before and after pictures after receiving two courses of treatment of ipilumimab with a significant response in the lungs, which is ongoing therapy after two years.
We’ve also seen responses in some unusual places. One place that a lot of our VEGF targeted patients fail is in the bone. This is a patient, before and after, who had a response with a bone metastases you can see here (left scan), and actual healing bone (right scan), just a year later with treatment. That’s certainly an encouraging result for us.
How long do these responses last?
For this admittedly small group, it looks like the major responses for a majority of these patients who had a response, that response lasted over a year. Most who had a response still have that response at a year. Whether that response will continue or stop, when the drug is stopped, remains to be seen. That will be a very important question. But the good news is the patients can tolerate this treatment for a year or more.
In summary, the PD-1 antibody concept is very early, but it has displayed reasonable side effects at all doses we’ve tested, and we seen some anti-tumor activity in some patients with kidney cancer.
PD-1 Antibody Summary
At this EARLY point, BMS 936558 has displayed manageable side effect at all dose levels tested
Anti-tumor activity observed in a small number of patients with RCC
Responses may be durable?
16 patients added to this cohort-ASCO 2012
Responses in NSCLC
Trials launched in 2011 in RCC:
Dose finding Phase II study in patients with prior therapy
Biomarker Trial
Combination RX + VEGF TKI (Phase I)
Were these remissions, i.e., durable, or just responses? Will the patients’ tumors grow after we stop the drug? We don’t know that yet, but we’ve added 16 more patients to the study. We will present data at ASCO in two months (6/12), with more information on this anti-body soon. It is important to note that with this drug and for the patients on it and for the field of immunotherapy for cancer that we are we seeing responses for kidney cancer and melanoma, where we’ve seen immune responses before. It is quite important also that we are also seeing responses in lung cancer. Should that be true, that will bring a lot of energy into the field going forward, as lung cancer is obviously a much more common illness, with very few options available.
There were a lot of new trials launched in 2011. We’ll have a Phase II trial in 2012, including multiple doses, to find the best dose in this treatment and also in combinations with other drugs like Sunitinib to find the best combinations.
So for those who say, “Is there a role for immunotherapy for RCC?” I would say there’s been a lot of progress over the last 30 years in the field of immunology, and we can now better target immunotherapy, and it’s worth preserving.
Is there a role for immunotherapy for mRCC?There has been progress in the field of immunology in the last 30 years
Immunotherapy can be “targeted”
Immunotherapy is worth preserving Slide 25
There is a role for immunotherapies shown by survival curves like this; this is from the SELECT trial mentioned before. These are patients who responded to treatment, now out three years, off treatment. The 13% percent of these patients, 16 patients have that benefit which really achieves the patient’s goal, which is worthwhile to try to get for more patients. It is proof of principal that we can do this, but we need to do it for lots more patients. If we work on this, hopefully we can achieve Dr. Wood’s goal of more cures for kidney cancer, with targeted immunotherapy.
QED
Audience: Does the pathway of the targeted drug therapy have any impact on whether or not immunotherapy would have any effect on tumor growth or not? Different targeted therapies have different modes of blocking pathways. Would that have impact, or has your research shown any impact on different pathways.
Mc Dermott: “That is a very good question and not simple to answer. Many of the treatments I talked about, like the cytokines, like IL2 or interferon or CTLA-4 work on the patient’s immune system-we think ONLY, only, meaning they are boosting the immune system to an established cancer. For reasons we don’t completely understand, that is effective in some patients and not in others. In the case of the PD-1 antibodies, they may be acting on the immune system, and may act on the tumor as well. There is some evidence of that in the early research, as I mentioned with patients who have this barbed wire on the surface of their tumors, or have this pathway activated, or when this pathway is on, they may be more likely to respond to this approach. Meaning, when the barbwire is up, and you can block its activity, maybe you can lead to an effective immune response. And what that may say something important about the pathway, but it may also say something about the immune system’s response. The barbed wire, we think, is up, as a reaction, a survival mechanism for some tumors. That is one of the reasons that cancer is so difficult to deal with, that there are so many different ways the tumor can evade the treatments. That barbed wire, that PD-1 may be one of those protection mechanisms. So that means tumor turns on, the barbed wire is up when the immune system is there, you can’t kill it, but you can block the barbed wire, take these immune cells are right there and it can kill the cancer. This may explain why some patients have a benefit and some don’t. And we are now looking to see, if your tumor has barbed wire, whether you are more likely to respond to treatment. There will be a lot more information about that in the future. Good Question.”
Question: I wonder if you knew if there was a clinical trial going on for prostate cancer, believe it is called XPl 4(sic), and its for bone mets, and if you knew anything about it’s work with RCC.
McDermott: “Re this med and RCC,I don’t treat prostate cancer, just melanoma and kidney cancer. Is the drug you are talking about XL 184? This is a drug that is in early trials, and maybe Dr. Jonasch will talk about it and similar drugs. These drugs work in the blood vessels to attack the cancer. They target two proteins, VEGF, which you’ll hear a lot about, and another protein which is important, C-MET, called MET inhibitors. There has been interesting activity in prostate cancer with this drug in trial, and a very small trial we participated in Boston with this agent with kidney cancer patients. You will see more info on this drug at the ASCO meeting in June and the info will be public on May 16. ASCO publishes all its info, so you will be able to get your hands on the results from that very small trial in a very few weeks, which is good. It’s a drug that has promise, but it has some side effects that need to be managed. The fundamental question here is for the kidney cancer advocacy community, is it going to be tested in kidney cancer? We are still not definite yet, but we are pushing to test this class of drugs in kidney cancer, this particular drug. We are pushing sponsors to do trials, but they are most interested in prostate cancer. When those trials are to start and with kidney cancer, we are not entirely clear. We need to push them to keep developing these interesting drugs for our patients.”
ME: This is an extension of the question, as to how you choose the best patients who have the best chance of responding to IL2. Does the histology or the pathology, and frankly I don’t know the difference between the two, have a major impact, and can you expand on that?
McDermott: “Yes, I may have gone too quickly on that. We thought the answer was yes, and when it comes to big differences, clear cell versus non=clear cell, it does, meaning when patients come to us, non-clear cell cancer for IL2, we will say to them, ‘It’s not going to help you, or the chances are so small, that the harm or potential harm outweighs the help.’ So to answer one of your questions, non-clear cell histology, which is simply a medical term for ‘What does this thing look like under the microscope?’.
For non-clear cell histologies, we don’t offer IL2. Whether one of these newer immune therapies work for that class of patients, should be tested because there is hope. That is why I mention the lung cancer story, because if it can work in lung cancer, it might in one of these less common kidney cancer types. It may work for many other forms of cancer. So that is a hopeful thing and exciting. But to take it a step further, while we thought clear cell cancer was more likely to benefit, we also thought it was that certain types of clear cell cancer were likely to benefit. That is what we tried to prove in that trial, but we couldn’t prove it. Doesn’t mean it wasn’t so, we just couldn’t prove it. We haven’t improved out selection ability based on looking under the microscope in ways that we had hoped. We can do it a little bit, and that’s why the response rate went from 14% when the drug was approved to 25 % today, but it’s not enough, so patients don’t have to go through the side effects if they are not to benefit from the treatment.”
Question; I don’t know if I know enough to ask a coherent question, but this is related. Why would it be that certain tumor types or subtypes would respond to IL2 or not? Is it because their profile of cell surface markers that let the immune system targets them better?
McDermott: “That’s actually a very sophisticated question, and one that does not have a clear answer. It may be, one thing you mentioned, it may be that the immune system usually recognized proteins, usually proteins associated with infections like viruses or bacteria. So it may be, as you point, that there are certain tumors that have show these proteins to the immune system better than others. And then the immune system can detect these proteins and say, “This is something wrong here, let’s go kill it”. That’s one possibility, and we tried to prove that in our trial, because one of the proteins we looked at was the protein called carbonic anhydrase IX. We thought this protein was being recognized by the immune system and that might predict for benefit, but we couldn’t prove it. So many people suggested your theory, which was that these proteins are important, but we could not prove it in this trial. It doesn’t mean that there aren’t others that are important, we just couldn’t confirm it. It may also mean that there are certain aspects of the tumor, that even though it is recognized by the tumor, something is preventing it from dying under the strain of an immune attack. That has to do with how well a cancer cell dies under stress. There may be some that don’t automatically shut down when they are being surrounded, that’s part of it. There are also other important proteins that the tumor can make to avoid detection so the opposite of what you are talking about, that barbed wire analogy. These are proteins that the tumor can turn on, and act like barbed wire, so that when the cells are coming it, they are turned off. So there’s a variety of different theories and more than one aspect of that. It’s a fairly complicated story.”
Me; Back to CA IX, the fact that you expected that more of that would lead to greater response, you found the opposite to be true?
“No, we didn’t find the opposite to be true, we found that the folks who had CA IX protein on their tumors did well, or better than the old numbers. Those patients responded at about the 25%, but they did as good anyone. What was different was that the patients who didn’t have CA IX on their tumor did just as well. So that is why I said it was bad for the research, but good for those patients. We would have assumed, if we hadn’t done the trial, that to those patients, we might have said, ‘You don’t have CA IX on your tumor, no IL2.’ We did the trial to show that, we couldn’t. That means that going forward,, we should include those patients getting IL2.”
Me: I went on IL2, and I am a complete responder, and I had a relatively low level of CA IX, so I always watch that and wonder.
McDermott: “You are an example of why my research career is floundering,” laughing.
Me; Sorry, but it works for me, works for me!
McDermott: “I am very happy for you and for those patients on the trial. That is why you do the research. The CA IX story, and this was scary when I saw it, actually made it into the medical training literature. So if you were an oncology fellow, you learned that McDermott at Beth Israel and others said CA IX was important, and that high CA IX patients should IL2 .And then when I saw the results of the trial, I thought, O my gosh, this has become gospel, and is maybe not right. You are a perfect example of it, and it means we need to do more research into the area . You are an excellent plant could not have been better.”
Audience: Did you say that you have some non-clear cell patients on the MDX trials?
“Not yet. Most of them whose tumor type we knew all have been clear cell. But in some of the future trials there are small numbers of non-clear cell patients who will be enrolled. If there is any sense of activity, it may encourage study sponsors/drug companies to develop it in non- clear cell patients. They will not be excluded on trials going forward.”
Audience: So you your knowledge there is not one which is limited (to non-clear cell) for MDX 186?
“I haven’t seen a response in that category, since most of the patients are clear cell the assumption in the field is that clear cell benefits from immunotherapy, so when you try to prove a principal, they try to collect the patients most likely to benefit, so not to put people through treatment that will not benefit. But now that we have this proven—really not proven—but a hint of effectiveness, different types of patients are being included in the trial. For example, the trial which includes the addition of MDX agent with Sutent allows non-clear cell patients. Hopefully there will be more of those in the future. The good news is there is more than one drug company developing these antibodies, and I will include those in my talk this afternoon.
We don’t do all the work at our place, but I haven’t seen a non-clear cell responder at my place. I have seen responses with very aggressive tumors, that had sarcomatoid features, for example, but I haven’t seen one with non-clear cell. That does not mean that it has not occurred.”
University of Texas MDACC; KCA Patient Conference; April 14,2012
Treatment Options for Patients with Non-clear Cell Histology
Thank you all for coming, and thanks to the KCA for sponsoring this, which has become a yearly event. So why this talk? The short answer is that regrettably, most of the trials if not all, recruit patients with the conventional histology, that is clear cell RCC.
But up to 20% of advanced renal cell carcinoma patients have these rarer types. That is not one type of tumor, but a diverse group of tumors. It’s not one disease, but heterogeneous diseases. I’d like to show you what has been done so far, and a glimpse of hope going forward.
You heard this morning about conventional type clear cell renal carcinoma, the most conventional; about 75-80% of patients with advanced RCC have this type. But about 20% have these diverse histological subtypes, with papillary 1 & 2 considered about 15%. Of patients without metastatic disease, who get just a nephrectomy for a primary tumor, it is estimated that about 10% will have papillary type 2 and about 5% will have type 1.
In my experience, when patients have recurrence after a nephrectomy, or present with advanced disease at initial presentation, the majority have the type 2 papillary.
Chromophobe is less common than papillary, is indolent, is less aggressive, and it progresses more slowly than the other. But when it is metastatic, it is incurable.
Collecting duct is another aggressive type non clear cell RCC, and renal medullary is a very close type, very similar histologically. However, it is unique in that it affects African-Americans, typically at a young age, who have the sickle cell trait.
Translocation is a newly diagnosed, or a newly recognized entity that is mostly present in young people, adolescents and young adults. We are now conducting molecular research on this unique entity.
There will be about 5-7% patients who will have this report signed by the pathologist, classified as unclassified RCC. This is really a waste basket diagnosis, as it reflects our inability to pinpoint the diagnosis, so “unclassified”. As our molecular insights advance, we will be able to classify the unclassified into more unique and distinct types. There are some rare cases, mucinous tubular and and spindle cell, TS thyroid type. Oncocytoma is usually benign, rarely metastasizes but it is one of those non-clear cell types also.
I added sarcomatoid dedifferentiation because it presents challenges to the treatment of patients with this dedifferentiation. Sarcomatoid occurs with all subtypes of RCC, the conventional clear cell type and non clear cell type. It portrays an aggressive behavior.
This is what papillary Type 1 looks like this under the microscope. This is an inherited syndrome that is characterized by germline mutation of the c-MET oncogene. It is characterized by considerable activation of the c-MET receptor. It is estimated that about 10-15% that are sporadic that are reported as papillary type 1 will have this mutation in the tumor .
The other papillary type 2 is also an inherited syndrome, also characterized by the germline mutation of a tumor-suppressor gene, the fumarate hydratase gene. Individuals that have this, in addition to renal cell carcinoma, have leiomylomas. Females have leiomyomas of the uterus; both sexes will have leiomylomas of the skin. They are referred to as HLRCC hereditary leiomyoma RCC. Sporadic tumors are obviously much more common in type 1 and type2 papillary rcc and the molecular knowledge about this, the molecular characteristics are not well characterized.
This is Chromophobe RCC; usually indolent, compared to the others, unless it is shown with saracomatoid features, and then it becomes virulent. There is an inherited syndrome associated with this, called Birt-Hogg-Dube syndrome, and there is a mutation in BHD genes: follicular is one of these.
Collecting Duct carcinoma of the kidney is highly aggressive, and it is a disease hybrid between renal cell carcinoma and transitional cell carcinoma TCC of the pelvis, which behaves like bladder cancer. You will see features of the RCC and TCC in patients that have this tumor. It is invariably an aggressive type of cancer and invariably presents at an advanced state. Renal medullary RCC is very closely associated with collecting duct, and affects young African Americans with sickle cell trait.
This is what unclassified RCC looks like under the microscope; with refinement of our technology we will be able to sub classify more the unclassified.
Translocation RCC is typically a disease in young females. Patients, young women and adolescents often present with advanced disease, with extensive lymph node metastases. The TFE 3 protein product of translocation has been studied.
This is what the sarcomatoid RCC looks like, and again it is associated with both clear cell and non-clear cell RCC histologies. Chemotherapy plus targeted therapy trials are ongoing but prognosis remains guarded.
Outcome of Patients with Advanced nccRCC
This is historical data, from the pre-targeted therapy era, when chemotherapy, interferon and interleukin 2 were the mainstay of therapy of patients with RCC. This is a retrospective study from the Sloan Memorial in 64 patients with non-clear cell histologies. The majority were reported as having collecting duct, then chromophobe, papillary and then unclassified. The median survival was about 2 ½ years in patients with chromophobe RCC, but worse in patients with collecting duct and papillary, and very dismal median survival with advanced papillary. Again, this is pre-targeted therapy.
We look at our own experience. These Kaplan-Meier curves represent patients treated;, the ones here (on the upper line) were treated with conventional. This is group (on the lower line) with the non-clear cell, the non-conventional. Survival is about 10 months median with the non-clear cell vs patients with clear cell. Again, patients treated in the era of immunotherapy.
Current Therapy of Metastatic Non-clear Cell RCC
So what about the current therapy of patients now with advanced non-clear cell RCC? I think that you may already have heard about this earlier from speakers.
Temsirolimus was tested in patients in a phase III trial, with advanced poor-risk patients, with advanced RCC, and with multiple risk factors such as poor performance status, anemia, hypercalcemia, and high serum LDH. Patients were randomized to receive either Temsirolimus, the mTOR inhibitor given intravenously weekly versus interferon as a comparator, or the combination of these two. Survival was the primary endpoint of this study. Of these patients, 20% had non-clear cell RCC histologies. Results were in favor of Temsirolimus with a median survival of 10.9 months with Temsirolimus vs 7.3 months median survival treated with interferon. This is an improvement of 49%. So you can say that for patients with non-clear cell histologies with poor risk factors, that Temsirolimus is a reasonable option as first line therapy.
This is a retrospective study conducted and published by the French and Cleveland Clinic, with investigators looking at the Sunitinib and Sorafenib. (Sutent and Nexavar) The majority of these patients (41 or 77%) had papillary, and 12 or 23% of patients with Chromophobe. The take home message on this retrospective analysis is that there was no central pathology review to really confirm that in fact, these patients had the reported pathology. Also, there was no central independent radiology review to confirm the responses. But the investigators reported a decent median progression free survival in patients with papillary, 7.6 months, but obviously shorter than what we see in patients with conventional type RCC. For chromophobe, the median PFS was even better at 10.6 months. Retrospective studies and again, patient selection biases are inherent in this.
The French conducted a Phase II trial with Sunitinibin papillary RCC. The majority of these patients had type 2, the most frequent type of non-clear cell patients with advanced disease. They observed only one patient achieving a partial response, 1 among 23 with type 2. None of the five patients with Type 1 had a response.
The Sloan Memorial group published their experience. This was a single arm phase of the trial, but unfortunately was closed to patient accrual prematurely, due to slow accrual. That brings up the point about the importance of patients’ participating in clinical trials. If we don’t really have robust participation in trials, we end up with trials that take a long time and many of them close before the end point is realized. Thus we really cannot make robust claims about the results. But among 22 evaluable patients, 8 had papillary, 5 unclassified and 10 were reported as having others. Only one patient had a positive response; that was one with unclassified rcc. The median PFS was just 5.5 months, basically half of what we would expect with patients with conventional cell histology. In patients with papillary, the median progression free survival was 5.6 months.
We at MD Anderson conducted our own study with Sunitinib. With 57 patients, this is one of the larger Phase III trials of Sunitinib–or any targeted drug in non clear cell RCC. The median age was typical of trials, about 60. We have different risk groups, good, intermediate and poor. Two-thirds of our patients had prior nephrectomy and we allowed prior systemic therapy. Eight patients had prior systemic therapy. We did not exclude patients with brain metastases, if the brain metastases were controlled.
HISTOLOGIES
This is the breakdown of the different histologies of the patients involved in that trial, with papillary constituting about half of the patients, 27 of the 57. Eight had unclassified, 7 had sarcomatoid, 5 chromophobe, 4 renal medullary and 2 collecting duct.
And there was one each of these rarer tumors. (slide reads tubulocystic, translocation, thyroid-like follicular carcinoma and mucinous/tubular/spindle cell.)
This is a summary of the efficacy data with the median follow up of 21.7 months. We observed 5 responses, less than 10%. Two of these responses were in chromophobe 2 of 5, that is, 40 %. That seemed to mirror the experience with conventional histology, and there was one patient each that had response, 1 of 25 in papillary, 1of 8 unclassified, 1 of 7 sarcomatoid. The important point to mention about this trial is that all the slides–the pathology specimens–were reviewed by one GU pathologist and all the scans, baseline and subsequent scans throughout therapy were reviewed by a single, blinded radiologist. So we are pretty confident of these results we report here.
The progression free survival and the overallsurvival of this data are in this slide. For the 55 patients evaluable for response, the median PFS was 2.7 months, absolutely very disappointing. You can see that the confidence interval is quite narrow, meaning we think that this reflects reality. For the 25 patients with papillary RCC evaluable for response, two were not evaluable for response. The median response for PFS was 1.5 months, again, a narrow confidence level.
For all 57 patients, the median overall survival was 16.8 months, perhaps reflecting maybe patients lived longer because they received maybe some subsequent therapy that they benefited from more than they benefited from Sunitinib. For the patients with papillary RCC, the median overall survival was 12.5 months.
The progression free survival and the overall survival of this data are in this slide. For the 55 patients evaluable for response, the median PFS was 2.7 months, absolutely very disappointing. You can see that the confidence interval is quite narrow, meaning we think that this reflects reality. For the 25 patients with papillary RCC evaluable for response, two were not evaluable for response. The median response for PFS was 1.5 months, again, a narrow confidence level.
For all 57 patients, the median overall survival was 16.8 months, perhaps reflecting maybe patients lived longer because they received maybe some subsequent therapy that they benefited from more than they benefited from Sunitinib. For the patients with papillary RCC, the median overall survival was 12.5 months.
Phase II study of Everolimus in Advanced Papillary RCC (RAPTOR)
There is now an ongoing trial, the RAPTOR study, with Everolimus, the mTOR inhibitor mentioned earlier. It’s occurring in Europe at multiple sites, and is a single-arm study of Everolimus in patients with papillary RCC. The primary endpoint of the trial is progression free survival at 6 months, and secondary endpoints are disease control rate, objective response rate (ORR), and median progression free survival (PFS) and safety.
Randomized Phase II Trial of Everolimus vs Sunitinib
There are two phase II trials of Everolimus versus Sunitinib, led by Duke and recruiting patients from Canada and the United Kingdom and one of our own, led by our institution with contributions from the Harvard Consortium.
A Phase II trial of Everolimus vs Suntinib in Non-Clear Cell in MDACC
The two trials are very similar in design except the Duke study–the ESPEN trial–does ot have a cross-over at progression with first-line therapy. This is the schema of treatment of the trial ESPEN, with Everolimus vs Sunitinib in prospective evaluation with patients with non-clear cell RCC. Patients with non clear-cell RCC after stratification, whether they have papillary or the other non clear cell subtypes.
A Phase II trial of Everolimus vs Suntinib in Non-Clear Cell in MDACC
The two trials are very similar in design except the Duke study–the ESPEN trial–does ot have a cross-over at progression with first-line therapy. This is the schema of treatment of the trial ESPEN, with Everolimus vs Sunitinib in prospective evaluation with patients with non-clear cell RCC. Patients with non clear-cell RCC after stratification, whether they have papillary or the other non clear cell subtypes,will be randomized to receive either Everolimus 10 milligrams a day or Sunitinib at the standard dose and schedule, 50 mlgr/day, four weeks on, two weeks off. They stay on therapy until they have progressive disease. At progression, they cross over to the other agent that they did not receive as first-line therapy.
Therapy of Papillary RCC; A New Way Forward?
Now moving forward. I hope the future will be brighter than what I showed you. There are a couple of interesting trials that I would like to present to you, what hopefully what the future will bring.
EGFR is being recognized as an important pathway to block several malignancies, epithelial malignancies, and kidney cancer is one of them. Evidence for EGFR over-expression or aberrant function has been reported in many of these epithelial malignancies.
Rationale for EGFR Inhibition in RCC
And there is a rationale for EGFR inhibition in RCC. This was from pre-clinical in vitro work in RCC cell lines. This was work done by Dr. Mendelsohn, our former president here, where they transfected VHL into VHL-negative cell lines and showed that restoration of the response to the antibody to against EGFR, the C225 antibody or Cetuximab was blocked the tumor growth, indicating that presence of wild-type VHL is required for effective EGFR blocking.
Phase II trial of Erlotinib in PRCC
That constituted the hypothesis for this Phase II trial, conducted by South West Oncology Group, published three years ago. They had 52 patients enrolled from 27 SWOG sites and 2 ECOG sites, seven of those 52 patients were ineligible for different reasons. Only 45 patients were evaluable.
Efficacy Median Follow Up
And this is the efficacy slide, with a median follow up of 21 months. There were 5 partial responders, four were confirmed, one unconfirmed. There was an 11% response rate with a wide confidence interval, as you see. (Wide confidence interval means less confidence in results)
EfficacySecond Endpoint OVERALL DISEASE
The overall disease control rate, a second endpoint of the study, and that included partial responders as well as patients with stable disease and this was 64%. The probability of freedom from progression or treatment failure at six months was 29%. The estimated fractions at 2, 4 and 6 months of patients who were stable or responding were 71%, 44% and 31%, respectively.
Overall Survival
Overall Survival at six months was estimated to be 87%, and median overall survival estimated to be 27 months. This is pretty encouraging, but again, a single-arm study of 45 patients, where you could bring up some patient-selection biases.
Study Limitations
These are the study limitations. They did not look at tumor grade. We know very well that papillary RCC is not one disease, as I mentioned and that patients with tumors which have high grade have more aggressive disease than patients with lower grade.
They also did not differentiate, did not characterize how many of those patients of the 45 recruited had Type I or Type II. There was no comment on what second-line therapy these patients might have received later after they received Erlotinib on this trial that could have confounded/compounded the survival and showed the survival to be better than what we have been accustomed to seeing. No mention of how many patients has prior nephrectomy or metastatectomy prior to enrollment in the trial. There was no correlation at all between EGFR expression with PFS or OS. And again, there were several patients who did not have central pathology review.
Erlotinib in RCC
As to Erlotinib in papillary RCC, Erlotinib appears to have some activity in papillary RCC. Overall, Erlotinib is a well-tolerated therapy, but is inhibition of this pathway beneficial to all patients with papillary RCC? That remains to be seen. Which subgroups of papillary would benefit most from the EGFR inhibitors? I think the story is similar to the story with non-small cell lung cancer, adenoma carcinoma of the lungs, where EGFR mutation has been linked to faster response among these patients. Which molecular markers will be predictive of response? We wait to see. Only through larger, prospective, randomized trials, will we be able to answer many of these questions. We need an ongoing, a future trial, looking again at Erlotinib (Tarceva) in patients with papillary RCC.
The C-MET Signaling Pathway
Now an interesting pathway is the C-Met pathway. This pathway seems to be operational, operative in some patients with papillary RCC. You see that hepatocyte growth factor is the ligand that signals through the receptors–the MET receptor–and causes down-stream effects. There are several agents in the clinic in phase I and Phase II that are targeting this pathway. This is an antibody (referencing AMG 102) against the hepatocyte growth factor, by AMGEN. There is another drug similar to this that targets the ligand, that is from AVEO and then there are several of this small molecule tyrokinase inhibitors that block the pathway here, intracellularly. I will focus now on one called Foretinib, XL880.
Phase II and Biomarker of the Dual MET/VEGFR-2 Inhibitor Foretinib in PRCC
This is a phase II trial that was conducted at multiple centers in the US. There was a biomarker initiative in this drug to study the effectiveness of the MET and how it was modulated and MET correlated with outcome.
We have already covered that the oncogenic events in PRCC are unknown, but do not involve the VHL-HIF-VEGF axis. Activating mutations of the MET gene have been identified in hereditary PRCC and about 10% of sporadic PRCC. Seventy five percent of sporadic PRCC may have duplication in the chromosome 7, at the location of MET, which enhances MET signaling.
Foretinib
What is Foretinib? It is a multi-tyrokinase inhibitor, and predominately blocks two pathways that may be critical in patients with papillary RCC, the C-MET pathway and the VEGF-R2 pathway. It was shown to have activity in xenograph models and in a phase I trial, two patients with PRCC had a durable partial response. One lasted more than forty-eight months. Based and encouraged by this, and on the rationale of blocking the MET pathway in papillary RCC, a phase II trial was then conducted.
Study Design and Treatment
This is the study design, the treatment plan for Foretinib. There were two dosing cohorts, one intermittent with 240 milligrams a day, given every five days for two weeks, and a daily dosing of 80 milligrams a day. The important thing about this design and its design in this trial is that patients were stratified by whether they had evidence of germline mutation of the MET oncogene or if they had other MET pathway aberrations such as somatic MET mutation, or duplication of chromosome 7 and/or 7q31 amplification. The study was designed to have at least 30 patients per dosing cohort.
Study Endpoints
The primary endpoint was objective response rate, and the secondary endpoints included progression free survival, overall survival, safety and tolerability and pharmacokinetic and pharmocodynamic markers, and the correlation of the MET status with outcome.
Primary Endpoint ORR
This is a summary of the efficacy, looking at the objective response rate. Thirteen point five percent had partial response; it was the same with the two cohorts, with intermittent dosing or daily dosing. Duration of the response was a year and a half, and 88% of the patients had disease stability, either partial response or stable.
Secondary Endpoint: PFS
Looking at the Kaplan-Meier curves of progression free survival, we see in blue the overall cohort of 74 patients, in yellow those receiving intermittent dosing and in red the patients treated with daily dosing. As you can see, compared to what we discussed earlier with Sunitinib and others, this is very encouraging, to have nine months of progression free survival in these patients.
Secondary Endpoint Overall Survival
In this slide of secondary endpoints, the median is not reached across both cohorts, and about 70% of patients were alive at one year.
Tumor Shrinkage in 50 Out of 68 Patients
This is a waterfall plot on the right, showing best % change of tumor from baseline. You see that 50 of 68 of patients had tumor shrinkage. Even though the response rate was low and did not meet the primary endpoint that the investigators set, fixed at 25% to make it more interesting and move forward with this drug, but at 13.5% , this was about half of what they aimed at. When you look at the tumor shrinkage, I think this is impressive to see this in a disease where we have no established therapy.
MET Status and Outcome
Now I think this is very important slide, as it illustrates a proof of concept, that when you target a particular pathway that drives the disease such as the type I where you have the germline MET mutation, five of ten patients, that is 50%, had partial responses. When you look at sporadic cases, only one of the five or 20% of those with the sporadic MET mutation had partial response, and the others did not respond. So I think this represents a progress, a map forward, to try to bring this company to sponsor a large trial, testing this in a large number of patients.
I told you I would mention sarcomatoid because it presents challenges to our management of sarcomatoid RCC.
Phase II Doxorubincin/Gemcitabine
Just briefly, the backbone of treatment for sarcomatoid treatment remains chemotherapy. People have looked at adding target therapy. This is the backbone of the treatment, two cytotoxics. In this trial conducted by ECOG, published in Medical Oncology Journal lately, the response rate and efficacy were not very encouraging. Median PFS, less than four months, median overall survival, less than nine months with chemotherapy for these patients.
Phase II Sunitinib/Gemcitabine
There is an ongoing trial at the Harvard Consortium, looking at combining Sunitinib with Gemcitabine in patients with either sarcomatoid RCC, or poor risk disease. This was presented with preliminary results two years at ASCO GU. There was a 25% partial response in 3 patients, but again looking at the time to progression of 4.8 months and then there was a high toxicity, with 25% of patients dropping due to high toxicity. This is ongoing with a total of 80 patients accrued on this trial.
Phase II Trial of Gemcitabine/Capecitabine/Bevacizumab at MDACC
This is our own experience on this trial. We just recently closed this trial with 34 patients accrued, combining Gemcitabine and Capecitabine, two cytotoxics with Bevacizumab, a targeted agent blocking VGEF. Again, our results are in keeping, in the ballpark with other trials.
Summary
In summary, non-clear cell renal cell carcinoma presents diverse rare tumors, and unfortunately, still we have no established effective therapy. This is why I believe that patients with advanced non-clear cell RCC would be best treated on clinical trials, as I believe you heard Dr. McDermott say earlier. There is no place where this is more urgent than patients with non-clear cell RCC, because the other FDA-approved treatments that work with conventional clear cell cancer, unfortunately do not work as well in non-clear cell. But the point the importance of collecting tissue. This is crucial to advance our knowledge.
Pedro
I want to finish with a glimmer of hope as I always try to in these presentations, where we don’t always have that much good news. This is one of my patients from ten years ago. This patient had a conventional cell carcinoma with sarcomatoid, had his surgery in the Valley, came two months after his surgery with metastases to bones, lungs, and lymph nodes. I show you this scan of Pedro. Pedro came in with a large family, 15 members, in a wheel chair. He had compromised performance status, required transfusions weekly, he had constitutional symptoms, with weight loss and sweating. This was ten years ago when we did not have any of these therapies.
Pedro wanted to be treated, his family supported him and we treated him with what we had at the time. That was chemotherapy with F/U, Gemcitabine, and low dose interferon. As you can see from this slide scan to the right, from recently, Pedro is alive and doing well in complete response, ten years later. He is celebrating ten years’ anniversary beating kidney cancer with his family.
Acknowledgement
We salute you, the patients and the families. You are the heroes who inspire us to continue our research to make RCC a history. Thank you. (said with great emotion)
Questions from the audience follow:
I want to say it is good to see some of you, patients of mine and families, you inspire us. I want especially to mention Teresa and Matt. We wish you all the best. Matt keeps me updated; he is my best source as to what is going on in the world, whether it is on Wall Street or any countries. I am going to ask him to join our research group, we need people who are motivated, and there is nothing better than the spouse and the patients. So I hope
that our partnering, academic centers and people like you, the patients and families –I think we can partner and be a force to push Congress, to push the drug companies to support, to bring in new drugs, new therapies, that we badly need for our patients.
Matt: I appreciate your efforts, Dr. Tannir, and any help with papillary would be great, and XL880 is stuck in limbo and XL 184 I think represents a lot of promise for papillary and also clear cell, in making those medications, making them available for our patient group, for patients with clinical trials and off label, where they are approved for other types of cancer.
Tannir; “I don’t want to forget that when we partner, also with insurance companies, because I know you, many of you struggle. I’ve had patients with papillary, as Matt mentioned, and there are no clinical trials available right now, and they reject that, and I think that is unfortunate that insurance companies. This now politics, but insurance companies, when you have gone through all the standards of care, you think that there is drug that might help them and they deny that. But I think that we can, by joining forces, that we can hopefully make that important change.
Kidney Cancer Association National Patient Conference
Dr. Thomas Hutson, D.O.; Texas Oncology
April 14, 2012 Management of Toxicities Related to Systemic Therapy for Metastatic RCC
Summarized from transcript and video; edited for brevity; Many slides were text-only, so recreated to keep files sizes small. Slides recreated in bold lettering and this font to keep the files small.
To view the lecture, please follow this link; you may copy and paste it into your browser. http://www.youtube.com/watch?v=KuJoHPA8sww&list=UUv0VRYOltlNQJLCyNMN61Nw&index=45&feature=plpp_video Be aware that this is a personal summary of the lectures, and that I am not a medical professional; I am a patient, highly motivated to share the information from this KCA conference.
Dr. Hutson thanks the KCA for the conference and begins:
“The “Management of Toxicities Related to Systemic Therapy for Metastatic RCC” is the bane of our existence in RCC; Dr. Jonasch explained the drugs and their benefits earlier, but with benefits often come side effects.
About two-thirds of these side effects–the toxicities–are mild, and are managed by “supportive care”. This means using medications to ease the toxicities. About 1/3 of the toxicities are severe, and may require a dose modification, a dose holiday, stopping the medication for a few days. For most patients, when the medications are stopped, the side effects go away. Most are not permanent. But when toxicity becomes so severe that it affects quality of life, such that we have to withhold that medication, we may move onto another kind of therapy.
Early recognition is very important. I cannot predict if a patient will develop a toxicity and who will not. We think about that from the research perspective, look at it from a genetic perspective. Studies in the medical literature show that patients’ genetics can affect the patients’ toxicity to the drug. Those studies are called pharmacogenomics or pharmacogenetics–things that make an individual patient or a group of patients more susceptible to a toxicity.
These drugs are approved and used around the world and other populations have different toxicities than patients in the US. Asian populations have more severe hematological toxicities, lowering blood counts than we see in US or western European patients. Clearly there is something that is genetic, a so-called pharmogenomic abnormality. Continued research in that area will help us understand that and predict who is going to have those side effects, and let us choose drugs accordingly.
Early recognition of toxicities is the key to avoiding severe toxicities and avoiding dose reductions. When I start patients on these new therapies, I generally see them every 2-3 weeks for a few months. Thus, we can get a handle on side effects, and have a plan, and intervene as needed. Most side effects manifest in first couple of months of therapy, and are often chronic, ongoing. Once we identify them as potential problem for that patient, then we have a strategy. Then I see that patient less frequently, every 4-6 weeks.
I do encourage the doctors–the community oncologists—to do the same, give early aggressive management of the side effect. But the patient or caregiver needs to pick up the phone and call the doctor or doctor’s nurse early when you have a side effect.
We must also consider long-term effects from these side effects, because patients are living longer. With these agents, used in sequence, patients are living 3-5 times longer than they were just a few years ago. Some patients stay on them for years. One man in my practice has been on Sutent for eight years; there are side effects that he will live with for a long time. These therapies have only been available for 5-6 years, and we are just now learning how to utilize them and their toxicities.
Let’s start first with the VEGF inhibitors, and follow with the mTOR inhibitors. The VEGF inhibitors, include Avastin (bevacizumab), an antibody treatment given by IV, and the TKIs, oral drugs, Sutent (Sunitinib), Votrient (pazopanib), Nexavar (sorafenib) and Inlyta(Axitinib). Their similar toxicities are called class effects.
The effect we see in clinic and most often reported by patients is fatigue. Next are skin/hand foot sores, mouth sores, and diarrhea–daily monster diarrhea. Cardiac concerns, the biggest being hypertension; patients’ hemorrhagic effects don’t seem very big, but epitaxis, i.e., bloody nose is very common.
What is Hand/Foot syndrome? This is palmar plantar erthrodysesthesia, a medical term for painful palms and soles of the feet. Often with calluses form on the pressure points, even cracking. It can get very severe, so the patient is unable to use the hand or the foot, unable to walk. One of my patients had an acute reaction with Nexavar and within three days came to me in a wheelchair. Thankfully that kind of acute reaction is relatively rare. This type of skin toxicity manifests itself in the first 2-3 weeks of therapy, reaching a peak in the first couple of months of therapy.
How do doctors talk about this? You have all heard doctors saying, “grade 1 toxicity, grade 2 toxicity” What does that mean?
To standardize reporting, we use a common language—Common Toxicity Criteria—from the National Cancer Institute, and incorporated into clinical trials. Every doctor can grade the toxicity of a patient in the same way.
Grade 1 would be the mildest toxicity, an eruption, and macular/popular eruption, a bumpy patch. Grade 2 would be the eruption, the bumpy, and now itching, covering less than 50% of the body surface, and Grade 3 would be that eruption, with itching and covering greater than 50% of the body surface area.
For Grades 1 and 2 we use supportive care, and topical emollients and such. For the grade 3 toxicity, very severe, we might hold the drug, let the eruption go away, and potentially, lower the dose.” If it continued or returned, we might change the therapy. Same for Hand/foot Syndrome; Grade 1, minimal changes. Grade 2, more blistering, more peeling, more pain, but not really interfering with your daily activities. Grade 3 is means it interferes with daily activities; you can’t use your hands or feet, affecting your daily life. Same thing; grade 1 and 2, supportive care, and at grade 3, we would be more aggressive.
There is also actually a grade 4 toxicity, which is very extreme side effects and a grade 5, usually considered a side effect that resulted in death.
For supportive care we suggest Udderly Smooth, Bag Balm, Aveeno, non-allergenic emollients or creams; good skin hygiene, good foot hygiene, avoiding shoes with pressure points in them, pain medications, traditional pain medications. Some patients use Solarcaine spray, which numbs the surface of the skin.
The next side effect, mucositis or stomatitis, those are mouth sores. We can do a mix of things–tap water or salt & soda mouthwash, that baking soda kind of mouthwash, change toothpaste, as some brands burn.
Lidocaine, such as dentists use can numb the mouth. We don’t want the mucositis to affect the patient’s ability to maintain hydration, the ability to eat, so again, monitor it.
Grade 1; mild side effects–use all the supportive care. Grade 3, very symptomatic, can’t eat, can’t drink, very difficult, and we must consider holding the drug or lowering the dose.
With Hypothyroidism fatigue is the major issue and with some of our drugs, fatigue occurs in 55% -65% of patients.
Fatigue has many possible causes, as it not one thing that causes fatigue in any one individual. Patients can have multiple causes at the same time, including the disease itself, anemia, lowering of the blood count from treatment, and pain medications.
We found the association of these drugs with low thyroid early on at the Cleveland Clinic. Many of these TKIs, at some level or another can affect thyroid function. Doctors need check thyroid functions in patients, especially if they have fatigue. This is something we can easily fix and put a patient on thyroid replacement therapy. Levothyroxine, a thyroid replacement therapy, may be used by a 1/3 or more of patients. Thyroid problems induced by these drugs is very common.
With thyroid issues we are constantly chasing TSH. It fluctuates constantly with these agents. My patients’ TSH is going up and down on their synthroid doses, very common. The graph shown here with Sunitinib therapy, shows the fluctuations of the TSH. If there is problem I am unable to control, I bring in a specialist, an endocrinologist.
Next is dysphagia–difficulty in swallowing–and diarrhea, which is a big side effect, so will review diarrhea.
Grade 1 diarrhea is an increase of fewer than 4 stools over baseline, i.e., normal. In medical texts, it’s considered normal to have a bowel movement about every 36 hours. But if you are used to about 1 or 2 stools per day, and it goes up fewer than 4 more stools than what you normally have, that would be considered diarrhea. Diarrhea is NOT based on liquid stools, but the quantity of stools. So even if you were having formed stools, if you were stooling–having more stools—several times over your normal, that is diarrhea.
Grade 2 is when your stools increase more than 4-6 stools per day, incapacitating. Patients may become dehydrated, so we think about giving IV fluids. Grade 3 diarrhea is the very debilitating diarrhea. With the frequency of the stools, patients are becoming very dehydrated and may need lots of IV fluids, perhaps even hospitalization.
As to treatment, we try over the counter medications, Imodium or prescription meds like Lomotil, or different kinds of diets, the BRAT (bananas, rice, applesauce, toast and similar) diet, different foods. We get nutritionists and dieticians involved. We try to bulk up the food with fiber, with Questran (check with doctor), Fibercon, different fiber products, from over the counter. There are medications that the doctors can try, things like Octreotide or ?????, Sometimes we give pancreatic enzyme pills, that patients with pancreatic issues use. But most patients have grade 1 or 2; we’ll try to control it, not eliminate it. These patients will have diarrhea every day, but controlled with Imodium and Lomotil.
Hypertension is a classic side effect, almost an on-target effect of VEGF inhibition. It is currently being investigated to determine if hypertension can be seen as a biomarker of activity against the cancer. That may mean that patients who develop high blood pressure while in therapy may have a better chance of response to the therapy than those who do not.
We tell other doctors not to lower the dose of the cancer drug, as that is a good sign. Keep that going, but treat the high blood pressure. Do that with blood pressure drugs, the kind patients are already on.
If I have a patient who that is having difficulty, and we are using 2 or 3 blood pressure drugs, I will refer him to a nephrologist, a kidney specialist, who specializes in high blood pressures issues or a cardiologist to help me. But in general, it is very rare to find a patient who cannot be on these therapies due to blood pressure issues. If the patient is already on blood pressure medications, he is going to have troubles down the road. We identify that before starting the therapy, be proactive. Have the patient check their blood pressure daily, keep a diary, review that, have a plan so they can stay on their therapy.
Epitaxis–bloody nose seems to happen quite a bit, especially when seasons change. The listed medications don’t have direct effect on the mucosal lining, but may when patients have inflammation., if they don’t make the blood is more thin. We use bedside humidifiers, Vaseline in the nose, nasal steroids and different agents to try to control it. I’ve only had one or two patients who had a major problem.
If you are predisposed to hemorrhoids , there may be more bleeding than usual. Try the topical products here, like Preparation H. Gingival bleeding, bleeding from the gums when you brush your teeth. Key thing that will interest surgeons is wound complications. If you are to have a surgical procedure, tooth extraction, or a surgical procedure that normally considered minor, you have to be concerned there could have complications with bleeding. Sometimes we’ll have the patient hold the medication for a few days before a minor procedure.
With a major surgical procedure, the literature is very controversial about the length of time, generally a few days, but that is at the discretion of the surgeon, and their comfort level. You would resume the medication once there was appropriate wound healing. Usually the surgeon will visit with you a week or 10 days, and remove staples and that would be a good time to resume.
A lot of side effects and it sounds bad, but I share some hope here. Tolerance may develop with long-term use. This is information from Nexavar from the original trial. The first, HFSR, the hand/foot syndrome is shown with the axis as cycles, 1-5, a month of therapy. The high peak that patients seem to have in HDFS is in the first cycle and fewer as the weeks go by, they develop resistance. Same with the skin rash; same with diarrhea, hard in the first cycle, more controlled in the end. The fatigue is similar. So a tolerance can develop, but you have to fight through the side effects.
Now about the mTOR inhibitors. We have Torisel or temsorilimus, a IV weekly medication and Afinitor or everolimus, the oral medication. Just as with VEGF inhibitors, these have class effects associated with both.
We see fatigue, skin rash, but no hand/foot syndrome. It’s not that severe life/quality of life syndrome that we see with the VEGFs inhibitors. You can get a mucositis, less severe that the VEGF inhibitors or diarrhea, but that is essentially it. You do not get the high blood pressure issues as with the VEGF inhibitors. Generally patients feel that the mTOR inhibitors are more tolerable, less difficult, less severe side effects than the VEGF inhibitors.
Unique about this class are hyperglycemia–raising of the blood sugar and elevation of cholesterol. If you have diabetes while taking mTORs, you may have to adjust up your diabetes medications. If you don’t have diabetes, it can sometimes cause a drug-induced diabetes, that requires medication, and is reversible upon stopping the drug. It is reversible side effect, but we have to plan for it.
Hyperlipidemia–elevation of cholesterol levels. I will check cholesterol levels every two months with patients on mTOR inhibitors. If we start to see it rise, we start them on therapy. Many of my patients are already on statins, lipid lowering medications, but it doesn’t seem much of a problem in them. But if a patient isn’t already on, they can develop this.
Hematologic effects. The mTOR inhibitors can lower blood counts, create problems with white blood cell counts, and infections, more than VEGF inhibitors. As a class, mTOR inhibitors are not just used to treat kidney cancer. Long term, and in Europe, they have been used as immunomodulators for transplant patients. They change the immune cells in the body to prevent rejection of organs. For patients with kidney cancer, we change doses, but they can create changes in the immune system and put patients to be at risk for infections, like pneumonia. Doctors have to watch for infections when on Torisel or Afinitor.
A unique side effect to this class is interstitial pneumonitis–inflammation of the lungs. If it occurs, and causes symptoms of coughing or shortness of breath, we need to consider discontinuing therapy. More details on that.
A skin rash with Torisel is usually on the torso. We use a topical crèams, emollients with Benedryl. We try to avoid using steroids, as this drug already has an immune effect and we don’t want to add to it. With a patient who has grade 2, less than 50% of the body affected in a skin rash, I sometimes get a dermatologist to help. If the rare patient develops the grade 3, with more than 50% body surface affected, I would have to consider stopping the medication.
Hyperglycemia has been seen with both the mTOR agents, and we need to monitor blood sugar. Sometimes that means making the patients get a blood monitor, to check their blood sugar medications at home, or start diabetes medication.
Again you can see elevations in triglycerides and cholesterol requiring patients to start on lipid-lowering medications. Those are both reversible when you stop the medication.
We talked about infection. There is a chance of infection with the mTOR inhibitors, so we need to be on alert for that.
Seen here are CT scans of interstitial pneumonitis: in month five there was a development of this nasty-looking infiltrate in the CT scans. That scares everyone when we find this on a CT scan. It could be ones, one; an atypical pneumonia, two; interstitial pneumonitis, a drug side effect, or the cancer. Sometimes, we have to refer patients to a lung specialist for a bronchoscopy to determine what it is. In this case, it was a drug effect, not an infection, and it was not cancer. It was the actual drug inflaming the lungs.
They stopped the drugs, they gave a little burst of steroids, it went away. Later they rechallenged the drug, and the patient went back on the drug, without further recurrence of the interstitial pneumonitis. If I had a patient with interstitial pneumonitis, I would find it very hard to put them back on the therapy. I show this to demonstrate that it is a reasonable side effect to expect, and it is reversible. It manifests itself as an x ray finding or as a cough.
The general recommendations are as shown. Call if there is any side effect which you are uncomfortable with. It is better to call early so you can intervene on it before it becomes a problem.
END of LECTURE: Questions follow from patients and caregivers.
Patient responses; Patient suggests Rock Alum in the case of mouth sores.
4 Archway macaroon cookies, twice a day
Capcesin for foot sores
Doctor agrees that patients have much to offer help with some symptoms.
Questions re coconut oil, to be used for mouth sores; Doctor had not heard of that.
Side effects do get better, says patient, asking about taking acidodolphodus; doctor agrees that pro-biotics, yogurt, is helpful, perhaps to change gut flora.
Question re Zometa as it is used with Sutent; Zometa has benefit in reducing skeletal related issues, and would be beneficial with all the drugs, says doctors.
As to difficult skin issues, doctors suggest the use of anti-fungals and consults with a dermatologist.
“Little about adjacent organ invasion. Most times when kidney cancer grows, it pushes things away. It rarely invades the liver, the colon, but if so, it is a really bad sign. Where there is locally advanced disease, with local organ invasion, those patients do the worst.
One of the challenges as a surgeon when the patient presents with local organ invasion in a CT scan is to determine if it truly exists. If we truly could identity those patients with local organ invasion, we might refer them for systemic treatment with a targeted agent before doing surgery.
We had 53 patients who had evidence on CT scans of adjacent organ invasion, but 30 did not have metastatic disease and 23 did have metastatic disease. Since 38% of those patients did not have adjacent organ invasion, what does that tell you?
That tells you that CT scans and MRIs are not the be all and end all of surgical planning. Those images are wrong 40% of the time. we were wrong, and if we doomed those patients not to get surgical treatment, and go on to get systemic treatment, it makes me wonder what their outcome would have been.
slide 51
This graph demonstrates that patients who have organ invasion do bad. In the absence of metastatic disease the median survival was 2 years and with metastatic disease the patients were dead within six months.
Slide 52 These are big operations, median blood loss of 2 ½ liters. Like to point that the big blood loss was not my case! But we do see complications with a mortality rate that is acceptable, so we can get patients through the surgery, but it is a big surgery
Slide 56a
:Again, the factors that predicted outcome for this group — patients who did not have true organ invasion, and again that feature that predicts outcome, presence of node metastases.
Renal Fossa Recurrence
Slide 56a
I will finish up with renal fossa recurrence. That means, after the tumor is removed, the patient recovers, the tumor grows back in the same place where the kidney was.
This retrospective study we did at MD Anderson seven years ago looked at 16 patients with locally recurrent RCC. Eight received neoadjuvant therapy and 7 received additional adjuvant treatment after surgery. Of the group of eight with neoadjuvant therapy, 50% were NED. The surgery alone group only 25% were NED, which shows a combination approach, that some form of therapy plus surgery is better than surgery alone.
Slide 58:A study out of Mayo Clinic basically shows the same thing. Patients who received surgery and systemic therapy did significantly better than those that received systemic therapy alone.
Slide 58: We recently published our study of renal fossa recurrence. We identified 54 patients who present with local recurrence, 69% of these patients received some sort of peri -operative systemic therapy. They all underwent surgical resection.
Slide 59: Again, this is a relatively aggressive form of RCC, with the occurrence free survival of about a year, but with aggressive surgical resection, these patients can live a long time. The median cancer-specific survival was more than five years.
Slide 60:
We tried to identify which features predicted outcome and found that those patients whose tumor size was less than 5 cm, and the ability to get a negative margin,meaning to remove the entire tumor with surgery– the absence of sarcomatoid features, a normal level of LDH in the blood test and a normal alkaline phosphatase, blood tests that we get; all these features predict outcome.
Nowadays when someone presents with a local renal fossa recurrence, we look at these features to see whether or not they are a good candidate for surgery, or if we should refer them to our medical oncologists for additional treatment.
Slide 62 is incomplete/ Wood’s comments follow: In summary, aggressive surgical resection, when feasible, still remains the best treatment for renalcell cancer. The role of targeted therapy agents in the adjuvant and neoadjuvant setting is unknown and should be protocol driven. Management of locally advanced disease remains a surgical challenge, but when done properly and by experienced surgeons, can give excellent outcomes.”
Surgical Management of Locally Advanced Renal Cell Carcinoma Part 3 of 4
Budd-Chiari Syndrome & Nodal Disease
One devastating complications of venous tumor thrombi is the Budd-Chiari Syndome. The thrombus gets so big that it plugs up the vein, plugs up venous outflow from the liver. Patients present with abdominal pain, ascites, i.e., fluid in the abdomen, edema of lower extremities, enlarged liver, and their liver function tests are all abnormal.
If we take these patients to the operating room, the mortality rate is about 80%. Because of this we no longer take these patients to the OR Instead we will embolize the tumor, cutting off flow of the blood to the tumor. For those patients that regress, we will take them to surgery and they do well.
It is not a very common presentation; we had six patients, two of whom were without evidence of disease after 3 years, using this approach.
NODAL DISEASE
There is a study where patients with localized RCC were randomized to either node dissection or not– to look to see if node dissection improved outcome. This trial showed that patients who had no dissection did no better than those who did not have node dissection. Many will use this in urology community to say that patients who have kidney cancer do not need to undergo node dissection in the absence of metastatic disease.
In a more recent update on this, again, those patients who had a node dissection did no better than those with a node dissection.
But one thing about this trial that troubles me and many in the urologic community is the significant percentage of patients who had very low stage disease. So it gets to the discussion of risk. If you study what you are doing in a low risk population where the frequency of the percent of expected adverse event is so small, you will never see a difference. The problem with this trial is that they need to focus on more advanced stage disease to see if node dissection really makes a difference with kidneycancer.
The group at Mayo did some very elegant studies which showed us where the positive nodes are. So now we go in and do a node dissection on a patient with locally advanced tumor, and we have a very defined area where we know the highest likelihood of metastatic disease is to occur. If we took out all the nodes, the complications would be enormous. We now are directed in where we go looking for nodes and remove them in that fashion.
Side 37 : The group at UCLA did a retrospective study and noted that if you did not have enlarged nodes, it did not matter if you took them out or not. Again, like the EORTC trial, but critics of this argue that it presents low stage disease. But one of the interesting things that did notice that in the patients with positive nodes, that if you took those nodes out they did significantly better. Indicating, even in the absence of systemic treatment, surgery could influence the biology of the tumor.
Slide 38
The group from Mayo identified features that predicted for positive nodes. These include high nuclear grade, the presence of sarcomatoid histology, large tumors or more advanced tumors, or the presence of tumor necrosis.
38a They assessed the primary tumor when it came out of the patient, and if there were 2 or 3 of these features, the risk of having nodal disease was significantly high that they triggered a node dissection. Now they use this prospectively to see if this does let us give better outcomes. This may give us the ability to predict who likely has positive nodes and therefore should undergo a node dissection.
Slide 39 This was a study that was done some years back, but it intrigued me. In patients that had even met and positive nodes, for example, mets to the lungs and positive nodes. Those patients do significantly worse in their prognosis than those without positive nodes. This suggests some adverse biology that is associated with positive node involved.
They also noted that if they could just dissect those nodes, again even in the presence of metastatic disease, they did significantly better than those whose nodes were left in place.
This is a study out of UCLA which shows that patients with metastatic disease do worse in the presence of positive nodes.
Slide 41a We recently looked at our experience (MDACC) with patients with metastatic RCC and positive nodes, limited to clear cell histology. We had 55 with positive nodes compared to 322 who did not. What we noted that those who present with positive nodes do worse than if they do not have them.
Slide 41b But you can see that if they undergo lymph node dissection, even in setting of metastatic disease, they did significantly better, almost a doubling of their survival as patients who did not.
Cytoreductive Surgery Prior to Systemic Therapy for Metastatic RCC
Slide 41c If patients do present with positive nodes, we aggressively resect them, as it significantly impacts on their ability to get treatment. So nowadays, when patients present for cytoreductive nephrectomies, if they have positive nodes, we aggressively resect them, as it significantly impacts their outcome, and their ability to go and get treatment.
Role of Aggressive Surgical Resection in Patients with Positive Nodes in the Absence of Distant Metastases
What about those patients that don’t have metastatic disease but just positive nodes. How do those patients do? We recently looked at our series of patients with positive nodes in the absence of distant metastases, and wanted to asses what factors predicted what affected outcome.
Slide 41d
Out of 3201 nephrectomies, we identified 2521 who did not have metastatic disease, and of those 68 had positive nodes. Surprisingly, we found, that in positive nodes–that the tumor has left the kidney and metastasized–and surgical patients still do pretty well.
Slide 42: There overall survival rate at five years is 37%. You might say, that is pretty low, but that is with surgery alone. But disease specific survival is 39% at five years.
slide44: But when disease recurs, it generally recurs early, at within the first year, but more than a third recur greater than a year out.
Slide 44a: And when patients do recur after this surgery, they usually recur in multiple places with metastatic disease.
Slide45
We wanted to look at factors that predicted for outcomes in these patients. So these are these are the demographics, (editor’s note; the video does not include these charts and slide, which are from the original, unedited video) the vast majority had good performance status, they had local disease, confined to the primary tumor and the overwhelming majority had clinically positive disease. This was not microscopic disease, rather big nodes you can see on CT scans.
What we noted, interestingly, in terms as predictors of overall survival those patients with papillaryhistology had a significantly better outcome, than those with clear cell histology. Those with only one node had a significantly better outcome than those with more than one mode.
When we looked at time to recurrence, again, papillary histology seemed to be a predictor of who would do well. So patients with papillary histology and positive node involvement, we will aggressively resect them.
Slide 45: The multi-variate analysis predicts for overall survival, and papillary histology, the number of nodes positive involved, the presence of sarcomatoid features and status all predicted outcome.
Regards of the time to recurrence, only the number of nodes involved and tumor grade were predictive of outcome in these patients.
(Slides are variations of the same information.)
Secondary Treatments
What about adjuvant therapy in these patients? I already told you that adjuvant therapy doesn’t work. In this particular group, 5 got adjuvant ttreatment and in those 4 patients, it recurred. The important thing is that 85% of these patients had good performance status at three months. What does this say? It means we can do an aggressive surgical resection and patients bounce back very quickly. If they need to go on to get additional treatment, even after this very large surgery.
So these are the feature that predict outcome; papillary histology, number of nodes, sarcomatoid features and ECOG performance status.
I will continue with “Adjacent Organ Invasion” in the next part of the lecture.
Surgical Management of Locally Advanced Renal Cell Carcinoma
Next is the management of more advanced disease, in patients who present with tumor thrombi, nodal metastases, adjacent organ invasion and renal fossa recurrence.
The first is venous tumor thrombi. This is one of the biggest operations that I do, as about 15% present with venous thrombi from their kidney cancer. These can be huge. This can be very complicated, as these thrombi can go up into the heart. We then have to put these patients on by-pass, open up their chests, stop their hearts and put them on a bypass, so we can take the thrombus out. We use TransEsophagealEchocardiogophy to monitor of the thrombus, to make sure that the thrombus does not break off.
This is a series that we recently published at MD Anderson, 605 patients with venous involvement, median age of 60 years, follow up of 24 months. 45% had no evidence of metastatic disease; conversely 55% obviously had advanced disease. The more advanced stage, the higher the risk of metastatic disease.
These are big operations; median blood loss is a liter and length of time is 3 hours, with complications inthe first 30 days for 25% of patients. Patients stay in hospital about six days. But even with venous involvement up to the heart, in the absence of metastatic disease, there is a median survival of five years, so even these patients can be cured with surgery alone. But once they demonstrate evidence metastatic disease, survival drops off dramatically.
Predictors of Overall Survival Slide
We looked at a variety of different parameters, won’t bore you with all the details. We looked to see what predictor survival for these patients and this is what we found.
Those patients who had clear cell histology actually had a more favorable outcome than those with non-clear cell. Those who had advanced grade, sarcomatoid de-differentiation, those who had peri-nephrectic fat, nodal metastases, distant metastases, all were associated with a more adverse outcome than patients with venous thrombus involvement.
Interesting was in our studies, not shown elsewhere in the literature, is that the height of the thrombus in the vena cava did not seem to matter. In other words if it was only in the renal vein, versus in the vena cava and that is at odds with the literature that is out there. It only seemed to matter when it went up into the heart, the red line at the bottom and with that, we saw a decrease in overall survival.
Tumor Thrombus and Survival
Our series are in concert with others, in regards to survival in the absence of metastatic disease that patients can have a long term durable survival, with about 60% with five year disease-free survival
Microscopic Positive Vein Margins Associated with Increased Local Recurrence & Metastatic Progression
One of the other things we noticed from our series that made me wake up was the concept of the vein margin. Of 270 patients, who had no evidence of metastatic disease, almost 20% of patients had cancer present at the margin of resection. When we resect the vena cava, we are obviously limited in how much we can take, unless we are doing a reconstruction, which is really fraught with complication.
(associated with increased metastatic progression.
But those with a positive margins, meaning they had cancer sitting at the edge of resection, where we cut the vein, had a greater risk of local recurrence, a higher Fuhrman grade. Those patients had a worse outcome, not surprisingly.
So now when we do these surgeries, we send the resection for a frozen section to be sure there is no cancer at the margin. If there is cancer at the margins, then we will do a reconstruction to try to reconstruct the vena cava to try to eliminate all the cancer.
Also in the literature that is out there that is a bit at odd with our series; here they noted that patients who had only renal vein involvement had significantly better outcome than those who had IVC (Inferior Vena Cava) involvement. There is some data that suggests that the height of the tumor in the vein is somehow related to outcome but that is not what we are seeing in our patients.
In this series, IVC (inferior vena cava) wall invasion, tumor size, fat invasion, nodal metastases, and distant metastases all were associated with an adverse outcome in patients with venous tumor thrombi.”
Dr. Wood continues his discussion of surgical management of “Locally Advanced Renal Cell Carcinoma” with Budd-Chiari Syndrome in Part 3.
Dr. Christopher Wood, of MD Anderson Cancer Center lectured at an April 2012t KCA patient conference on this critical subject. It is a technical discussion, highly important for the patient whose kidney cancer is not longer consider “small and curable” by surgery alone. For greater ease in following this, I have posted this in four segments. My comments will follow in a separate blogs. My hope is that the information is meaningful, so that a patient can learn enough to have a discussion with his/her doctor. Print out the information you have read and give it to the doctor to start that discussion. Some slides were principally text, so I have recreated some to keep the file size down; anything which was not readily converted to text remains as the best available slide.
Consider saying to your doctor, “Here’s what I have been learning, doctor. How does that fit into our plan for my treatment?” That tells your doctor know you are willing to learn and to listen, and to take an active role in your treatment decisions. Unless your doctor deals daily with many kidney cancer patients, he is unlikely to be able to keep up with all the information, ever changing, and ever more complex, about your disease. If the doctor is not willing to listen and learn from the leaders in the field…find another doctor.
Peggy: RCC Patient, Stage IV mRCC 2004; healthy today, thanks to HD IL2
“Outcomes for Patients with Locally Advanced Renal Cell Carcinoma”
Dr. Wood begins: “My first lecture is “The Management of Locally Advanced Renal Cell Carcinoma”. Slide 1
Stage is the most important predictor of outcome: the more advanced the stage, the greater risk that the tumor has spread, with distant metastases, making the disease incurable.
This is the staging system we use in 2012, where we stage tumors, assess regional lymph node involvement and look for evidence of metastatic disease. People get hung up on their staging, but this allows doctors to communicate about patients in the same language about how advanced one tumor is. With increasing stage, there is a more locally advanced tumor or metastatic disease.
Let us start with definitions. (Reads slides 2 & 3)
Adjuvant Therapy means some form of therapy– chemo, radiation, vaccine, whatever–after complete surgical tumor resection with the idea to decrease the risk of recurrence of disease. The benefit is that the patient has already had surgery before getting additional therapy, but the downside is that many of those patients may have been cured by the surgery and they may get treatment they don’t really need.
Neoadjuvant therapy is taking some form of therapy, whether chemotherapy, radiation, vaccine, etc. prior to surgery to the primary tumor in hopes the tumor may decrease in size, and decrease the risk of recurrence. The benefit is it may allow the tumor to shrink and make surgery easier. The downside is that the therapy may not be effective and not inhibit metastases, and the primary tumor would not regress, but progress during therapy.
Slide 4
Effective adjuvant or neoadjuvant therapy does not exist for kidney cancer in 2012
Any therapy must be developed in the context of a clinical trial setting, and including a placebo. The only way we make advances is to test what we do now with any advance in the future. And what we now know, as I said, is nothing.Patients have a hard time, with placebo trials. If you participate in such a trial, the treatment you are getting may not be good and the placebo arm, not so bad.
Slide 5 Who should get these therapies? Why not give them to everyone? Anyone taking the targeted therapies today knows the toxicity is significant, and you may treat a significant number of people who really don’t need the therapy. Then if nothing works, why not give it to anyone? Well, we are never going to make advances that way, so it is important that we continue to do research and focus on those who are highest risk for relapse. Should we give it only to those at a highest risk for recurrence? The difficulty how do we define risk, how high is high? So it’s not really clear.
Adjuvant Therapy: 2012
A variety of trials have been performed. Many patients have participated. They include radiation, embolization, energy ablation, a variety of different hormonal therapies, immunotherapies with interferon and interleukin 2, all having been used in an adjuvant setting. There have been a variety of vaccines preparations and we did a Phase III trial of thalidomide trial here. To date, not one ofthese therapies has shown benefit in the adjuvant setting. In fact, many of the patients on the treatment arms did worse than those who were not treated.
Slide 7 What about targeted therapies? That is also the great unknown where things stand with targeted therapies in the adjuvant setting.
Since 2006 there have been seven new agents against kidney cancer. It’s been a revolution. And to be honest, many have benefited from that advance. How do we use these agents in the context of adjuvant therapy?
Slide 8 There is a variety of trials recently completed or in accrual, ongoing. Tthe ARISER Trial used an antibody called G250 against Carbonic Anhydrase IX, and patients were randomized to get either antibody or placebo. This trial completed accrual many years ago, in fact, and we are still awaiting results which leads me to believe that is probably going to be a negative trial.
But this same agent has recently shown promise for use in PET scans for kidney cancer. You can use this as an imaging agent. The patient is infused with the antibody and linked to item 125, and it will show up on x ray, and may potentially detect micro metastases not visible on CT scans. This is actually undergoing FDA approval.
Slide 10
This is the ASSURE trial we conducted at MD Anderson. It is a randomized, double-blind phase III trial of Sunitinib vs Sorafenib vs Placebo. Patients underwent surgery, then were treated with these agents for 1 year. This trial was completed accrual last September (2011) and we are now waiting for the trial to mature to see whether these agents have any benefit in the adjuvant setting.
Slide 11
One thing that we did learn from this trial is that tolerance for the toxicity associated with targeted therapy in the adjuvant setting is not the same as in the metastatic setting. In this trial 41% of patients stopped therapy early, not because disease returned, or because they finished, but because of toxicity. I think it comes down to an individual assessment of the risks. If I told you that you have a 20% risk of your cancer coming back, versus your 70% chance of your cancer coming back and you are miserable on this therapy, all of a sudden 20% doesn’t look so bad.
My concern about this, because at the end of the day, if this trial matures and it is negative, will it be negative because the agents did not work, or because the patients could not tolerate the side effects. And too many patients stopped the trial early or had dose reductions. I’m afraid it is not going to be interpretable.
Slide 12 This the S-TRAC trial, sponsored by Pfizer, recently completed accrual. It’s randomized between Sunitinib with a placebo for one year. It is estimated results will come out in 2017. That’s the other problem with these trials. Are the agents we are testing now, will they even be relevant in 2017? No one knows.
Slide 13/12
There has been a real problem in accruing to this trial. In fact, we can’t even keep patients on Sorafenib for three years in treatment, never mind adjuvant setting.
Slide 13
This is a trial going on in the US, sponsored by Glaxo-Smith-Kline. This is called the PROTECT trial. Patients are randomized to Pazopanib (Votrient) or placebo for one year. This is primarily open to clear cell patients, here at MD Anderson.
SLIDE 15 A
This is the EVEREST trial, sponsored by the SWOG, going on around the US, with patients randomized to one year of Everolimus (Afinitor) or one year of placebo.
You can see that clinical research is actively ongoing to identify if these agents work in the adjuvant setting. But it is going to take more time to understand from these trials before we know if this is applicable in these setting or as with the other agents, if they remain ineffective.
Slide 16
One other concept we are testing at MD Anderson that I will talk about a bit more in the next talk is a neoadjuvant therapy, testing Axitinib in the neoadjuvant settings. Some in the audience have been on this trial, where patients receive Axitinib for three months and then undergo nephrectomy.
I would like to applaud the patients who participated in this trial. Like to give you an idea how this went the first time we enrolled a patient. Patient comes in with a tumor, curative with surgery, and we say, “We’d like to give you this agent, we don’t know if it will work. In fact, your tumor may grow and metastasize while you are getting this agent. If we took you to surgery tomorrow, we could probably cure you. What do you say?” It was really amazing. The first patient who enrolled in this trial was very brave. But since we have been able to show activity with this agent, enrollment has picked up significantly.”
Dr. Christopher Wood ends the first part of this lecture, with the next section about “The Surgical Management of Locally Advanced Renal Cell Carcinoma.”


 Slide 2: This is not to scale; it is 213 amino acids long and for the scientists in the audience, that is mercifully short, and it also has three exons in or three parts, or easier to study than most, but obviously still hard to study.
Slide 2: This is not to scale; it is 213 amino acids long and for the scientists in the audience, that is mercifully short, and it also has three exons in or three parts, or easier to study than most, but obviously still hard to study. Slide 3:
Slide 3:
 So the “blood vessel starving” are the five antiangiogentic therapies we currently have are listed here, and I am going to go through each of these in details.
So the “blood vessel starving” are the five antiangiogentic therapies we currently have are listed here, and I am going to go through each of these in details.


























































































")

































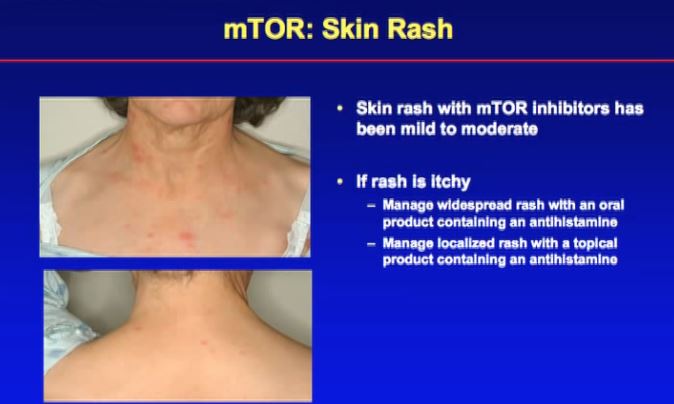






















































- A Randomized Double Blind Phase 3 Study of Adjuvant Sunitinib vs Placebor in Pts with high risk RCC")



