It’s bad enough to worry about having had a tumor, but now we are learning that the microenvironment of our own systems–and their microlocations–are important! What is next? And what is a tumor microenvironment anyway?
My own primary tumor apparently was quite efficient in spinning off its alien babies, the metastases which peppered my lungs. None of these ambitious invaders seemed to have found a happy home in my bones, so one could think that my lungs were a nicer neighborhood or microenvironment for my mets. It is bad enough to have the cancer on the move. Does this mean that mets in one place will predict mets in another?
To answer this question, it is helpful to understand how cancer cells move through the body and find their new unhappy-making homes. Happily for us, as the hosts of these unwanted and busy guests, the body does try hard to limit their invasive moves. And the presence of our healthy cells and the general brakes of our immune system do offer some protection. Editorial note here; It wouldn’t hurt one bit if you do everything you can to support your immune system, and make it efficient in keeping you healthy.
For cancers to grow beyond their original location, individual cancer cells have to escape the primary tumor. Think of tiny ships leaving earth’s atmosphere, pulling away from the tethers of gravity and the support mechanism inherent in the tumor environment. Then those cells must survive the ride through the blood or lymph system, which is really designed to break up the cells, before landing at a new and unknown site. Cleverly, there may have sent out certain proteins in advance to, to fertilize the ground of that new colony, but the seekers may never find that soft landing. And then those same cells need to support themselves, far from home.
Researchers tell us that tens of thousands of cancer cells can be shed into circulation every day, but less than 1/100 of one percent of them ever survive to relocate and reproduce. Lot of good things happen to stop that. And those darn cancer cells use platelets as shields against the vigilant immune system and recruit clotting mechanisms to strengthen their structures. Some might even take on characteristics of stem cells as camouflage.
Should that tiny colony of cells find fertile ground, they must survive many challenges before they can grow and cause any real impact on our systems. Researchers and patients are aware that certain cancers seem to have favorite metastatic sites, with lungs and bones the preferred new locations in kidney cancer. Just to make things more confusing, there are several ways that cancers grow, which seems to depend on the original source of the cancer. And there are local growth factors, quite normal and appropriate in the bones, which can be subverted into helping establish new metastases. It’s as if the cells looked around and found local cells ready to collaborate with the enemy!
But that same collaboration and the resources that this unholy partnership brings the new relationship gives an opportunity to prevent the invaders from settling in comfortably. Noticing the chemical welcome mats, researchers are aware of the possibility of “pulling that rug out from under” the newcomers, and making them less likely to set up shop in your bones or lungs.
They have been especially helpful in preventing bone metastases by using some agents that were developed not as anti-cancer agents, but to strengthen bones in general. Since breast cancer also moves to the bones, the use of these agents, bisphosphonates and others, is wide prescribed not only in the presence of mets in the bones, but to prevent them. Prevention of mets is an adjuvant therapy–another of those new words for your vocab test. Examples of these agents are Zometa and Xgeva, each with special characteristics.
In advanced RCC, where Sutent is being used, there are studies which show longer benefit, when Zometa is also given the patient. Zometa obviously makes it less comfortable for the mets, which may be tiny and unseen, or newly visible on a bone scan, less likely to continue to grow. And I am for anything that makes is hard for mets to grow, even if they are really still in the neighborhood.
Just as there are many factors which aid and abet the nasty mets to leave home and travel, and take on new disguises to evade the immune system, there are likely many more approaches to limit the welcome at the new desired location. One challenge is finding those, as is obvious, and more urgent is to understand when one’s targeted therapy is helping against metastases in one part of the body, only to have a new location be invaded by mets.
If you are getting benefit from one targeted agent, but new mets pop up elsewhere, do you stop the Sutent, and risk more mets in the original area? Do the new mets need a biopsy to see if there has been a change in molecular characterization which may direct the use of the next medication? Can you add another agent without undue side effects? None of these questions have clear answers, but a willingness to examine what it happening and how and where any mets might be made less comfortable in their growth patterns is critical. Wish it were simple, but it is not.
Probably the most talked about studies at the June 2013 ASCO in Chicago swirled around the newly released trials about PD-1 (Programmed Death-1) and similar. “What the heck is this all about, and why should I care?”, you may be asking. This is important as it shifts attention back to the original immune therapies that kept me alive (and many others) when there was nothing else to offer any hope in the olden days of the 1990s.
Though a number of targeted therapies have since emerged, and you have been hearing about them, there is new interest in the earlier and modestly successful immune therapies. I confess a fondness for anything described as an immune therapy, as I am alive–which I would NOT have been–without the first FDA approved agent against kidney cancer, high dose interleukin 2, brand name Proleukin.
The first new agents in the 2005+, the anti-angiogenesis drugs (not easy to pronounce,much less to understand) brought new hope to metastatic RCC patients. With the late diagnoses of many kidney cancer patients, we desperately needed hope. For about 14 years, HD Il2 (high dose interleukin 2) was the only game in town. Nothing else existed, so any patient lucky enough to hear about it, and not actively discouraged by the very “realistic” doctors, probably considered it. This is a hospital-based agent which revs up the immune system, so the immune system would go after the metastatic disease, at least for some number of months or years. That is why I am alive. Nothing else was offered and nothing else was available. Nine years!
Since that time the anti-angiogenesis drugs–translation: those that fight against (anti..) the creation (genesis) of angio (think blood vessels) drugs were approved. Think Sutent (sunitinib) and Avastin (bevacizumab) and others,. They have been the weapon of choice for oncologists and patients. Why is that? Though these drugs rarely offer more than some pushing back of the drug, decidedly welcome, they have rarely given more than some slowing or relief from the metastases, and always with some side effects.
For us old-timers, who faced only death, whether by efficient means or by surgical cut-and-pastes as holding actions, this was a tremendous breakthrough. For these options, even if only holding actions versus mop-up operations, we were grateful. We who had nothing previously were slightly scornful of those who complained about the side effects, as we were grateful to be around to have such effects. The Stage IV sufferer in 2004 knew too well that Stage V was a damn unpleasant journey and without a return ticket.
Now we have become greedy again, wanting more than the “stability” or “some shrinkage”, which I applaud. We want success and life, not holding actions. High dose interleukin 2 continues to offer that success to patients, but no one can predict which patients and which conditions that might be likely.
Bless those researchers who continued to wonder why kidney cancer and melanoma (and maybe non-small cell lung cancer) respond to some sorts of immune therapies, and what happens to make that happen and not happen. Those fine people have come to understand that the immune response which is revved up by HD IL2 has a complex set of “calls and responses” which either let loose the dogs of war/and immune responses, or fail to do so.
Most people understand that the body tries to protect itself from assaults, whether by poison ivy, bronchitis or cancer. The immune system responds, gives the body aches, pains, fevers, chills, etc. Think of flu and how rotten you can feel. Think also of old diseases like Black Death which stimulated the immune system so violently that it was the strong and healthy with good immune systems that succumbed to the immune response, dying with lungs filled with immune reactions and fluids. Only those with weakened systems and slower responses managed to live through the symptoms.
Obviously the body’s immune response needs a moderation, and not one that saves the village by killing it. All of this leads to an explanation of the newest immune therapies, now in clinical trials in RCC. You may hear about PD-1 and CTLA-1 trials, and how they may be helpful in kidney cancer, melanoma, and now in non-small cell lung cancer.
To understand all of this, it is helpful to think of a system of checks and balances, perhaps in an electrical or computer communication system. Just as every electrical impulse might be appropriate, it could also do damage by overwhelming the system, burning it out, or failing to meet the requirements to be able to answer a “send me” signal. So it is with the latest research on immune therapies with the PD or Programmed Death agents.
Keep in mind that the immune response is typically used against infections, and not generally against cancer. I assume that we cavemen needed more protection evolution-wise against infections and less so against the ravages of cancer, which seems to result from getting older and getting overwhelmed by changes/mutations in the body. (Not always, I know, but that is a discussion for later.)
T cells are supposed to react to a number of infections and such, and trigger an immune response to fight back against the “aliens”, such as cancer and ragweed. Just right amount of fight, and the body recovers. Too little, and you have the devastation of the Black Death, an over-the-top immune response.
The immune system is supposed to respond to handle the natural threats to the body, but not over react and set the system on fire metaphorically. It had built in checks in balances, as do normal cells. We see this everyday when our normal growing hair cells decide to stop growing and the hair fall out. Chemo patients struggle with the balance of killing all cells, with the faster-growing cancer cells being killed off first.
New agents have been developed that interfere with a signaling system that puts the T cells, the protective/fighter cells into action against cancer cell. This naturally happens, but the nasty cancer cells try to evade that process by interfering with that process. Not letting the body protect itself, by disguising itself as the evil twin, equally eager to live, as the good twin, the healthy cell, cancer interferes with Programmed Death. More next time…
And as Mae West said, “I like a man who takes his time.”…
If anyone can find a cancer event exciting, it is the ASCO annual meeting, at which thousands of oncologists present their studies and learn from one another. In the kidney cancer world, the “buzz” has been about “programmed death”–for the cancer cells, which we all prefer over that of our healthy cells.
This is a transcribed lecture, fairly short, to explain the immune therapies that may add to those weapons against RCC. Dr. Wolchok clarifies how this happens, with the agents interfering with the “Shields Up!” commands that protect the cell from what should be their programmed deaths. With appreciation to all researchers.
Peggy–Nine years of life free of cancer, thanks to the original immune therapy, HD IL2
ASCO Daily News June 6, 2013
Dr. Jedd D. Wolchok, MD PhD of Sloan Kettering Memorial Cancer Center
We now recognize that there are several pathways that constrain T Cells and the immune system from achieving a state of full and persistent activation.
One of those pathways is called the CTLA4 pathway and there was a medicine approved call Ipilumimab last year, that blocks CTLA4 for treatment of melanoma. There is another pathway, the PD 1 pathway which usually constrains the immune system in a different way. And PD 1 is also present on T cells in the immune system and it binds to a family of ligands, one of which is known as PD-L1 or PDL ligand 1.
In the ever-expanding a list of ways in which cancers try to evade the immune system, cancers have learned to express this PDL-1 ligand on their surface. By doing so, they actually cause the death of T cells that come close enough to them or PDL-1 to bind to PD-1 on the T cell surface. This ability of cancer cells to express PD L1 on their surface allows them to defend themselves against T cells that the body is trying to educate to see the cancer and to defend itself.
So the PD-1 pathway is active across multiple disease sites. Some of the earliest work done with anti-bodies that block the PD -1 pathway used an anti-body called Nivolumab. Nivolumab was used in a phase 1 clinical trial that was presented at ASCO last year, and additional data will be presented this year.
The data last year showed that the antibody Nivolumab blocks PD -1, and that it can cause regressions in melanoma, in kidney cancer and importantly, really, non-small cell lung cancer. It is not traditionally recognized that as a cancer amenable to immune intervention. But when you people talk about cancers that responsive to immunotherapy, melanoma and renal cell carcinoma come to mind.
Now I think with the data generated first with Nivolumab and now with another PD-1 blocking antibody called Lambrolizumab(MK-3475), these anti-bodies which block the PD -1 pathway are demonstrating activity outside the “usual suspects”, melanoma and kidney cancer.
This ability to affect multiple different cancer types is important, as it shows that immunotherapy is not a treatment for one particular kind of cancer,. It is a treatment that primarily targets the patient, Then it is the patient’s immune system that goes out and treats the cancer.
One of the most important characteristics of immunotherapy is its ability to induce durable and certainly there are many different types of anticancer medications which can cause a tumor to reduce in size, but the challenge has been and continues to be, how to get disease to regress and stay regressed. Tumors, because of their genetic instability, can find pathways to become resistant to these interventions such as chemotherapy or targeted pathway inhibitions.
Immunotherapy really falls into a different category. Again, it is not targeting the tumor itself. It is targeting the patient’s immune system. It is causing the patient’s immune system to respond to certain parts of the tumor cells that the immune system finds interesting and then to control.
We know that the immune system has the ability to remember, through to a population of cells called memory cells. Because the immune system is really a dynamic organ that cannot only sculpt itself around changes in the cancer, but also can remember what it has been exposed to in the past, we believe that durability is in fact a hallmark of response to immunotherapy. The first medicine to show us this in a meaningful way was a drug called interleukin two which was really actually developed now over 25 years ago and has led to the cure of some patients with melanoma and kidney cancer. That medicine is a hormone that causes the growth and differentiation of T-cells and patients who have a complete response to IL-2 and remain in complete response for at least two years don’t ever seem to recur with 10 or more years of follow-up.
We definitely need to learn more about the PD-1 pathway we specifically need to know whether it’s absolutely required for a tumor cell to express PDL-1 that on that surface to benefit from PD-1 or PD L-1blockade. It would be ideal, in fact, if a predictive biomarker that could identify the precise patient population who would benefit from that intervention. However, I think that is not going to be a simple as predictive biomarkers been for some of the targeted therapies, where it is mutation-present or –absent. Here PDL-1 is not just important when it was expressed on the tumors, but PDL-1 plays a role by its presence on antigen-presenting cells. So, in its normal physiologic role, the PD -1 pathway actually involves interactions between T cells and antigen presenting cells and by blocking cells–even if the cells doesn’t express PDL-1–one could imagine that a patient could benefit, perhaps not as likely as if the tumor expressed PD L1.
When I was diagnosed with kidney cancer in 2004, with a tumor that had pushed my kidney toward my belly button, and had filled my lungs with tiny white dots foretelling my death, I had one FDA-approved treatment offered me. It was that or nothing. And by nothing, I mean the big, metaphysical NOTHING. There was no way to nip and tuck away at my lungs to remove the tumors. It would have been like trying to salvage a sponge by cutting away the black fungus that grew throughout its nooks and crannies.
Systemic disease sounded more hideous than distant metastases. The one treatment–high dose interleukin 2–was already about 12 years old, and nothing better had come along. The rate of benefit was low, and many hospitals didn’t even bother to offer it. That is still the case today, with fewer than 90% of kidney cancer patients (and our melanoma counterparts) are told about it. Desperate patients whose disease could not be chopped out were the candidates, and I was one of them.
This was an immune therapy, described to rev up one’s immune system, just as happens when you catch a cold or have an infection. It’s pretty obvious that this worked for me, not just to keep be alive while fighting the diseases incursions. I am free of cancer, though I get a CT scan every six months, a search and destroy-if-we-find-anything mission. so far so good, and I may even be cured.
Me, seven –TEN–had to edit it, as I keep living– years after HD IL2 and healthy
No one yet understands why I responded to high dose interleukin, but this old and disrespected therapy has been the silent reminder of the possibility of turning cancer off in the body. New studies are emerging to support this approach.
Just days ago in Chicago, researchers presented information on related immune therapies that offer benefit to some patients, spotlighting HD IL2 and using immune response to conquer cancer. Not just to contain or to making cancer chronic, which is laudable in itself, but to conquer it. Why has it taken so long to use the success of HD IL2 as a beacon to light the way to increased study?
Some say that finding out that HD IL2 worked was plain lucky, but that does not carry the appreciation for the effort that went into it. Brilliant researchers led the way, but desperate patients of 25 years ago, having no options and fiercely determined to make sense of the devastation of this disease, entered clinical trials, With tremendous risks, no guarantees, and no fall back plans, some died. Others lived a few more months than expected, which equaled success at that grim time. Some lived without disease, their cancer conquered and vanquished. Brave and selfless people, to be admired.
Some new research on the dynamic signaling process that characterizes the growth of cancer has been emerging of late. Cancer grows by evading the immune system, sneaking under that exquisite alarm and response process, turning off chemical triggers that should remain on to block its growth. Learning more about that intricate system, a call-and-response process that is just now being understood has brought about agents to support the immune system.
Not just killing cancer cells faster than the health cells are killed–quick version of chemotherapy–these new agents interfere in the cancer growth. Whether the research will show that response is durable and lasting, as with some HD IL2 patients, is yet to be seen. But my hope is that this type of research will reinvigorate the interest in using the immune system to return many more patients to health, as was done for me.
PS A new lecture by Dr. Jedd D. Wolchok–blessedly short, though well-explained will be posted shortly. PD-1 Pathway. Watch for it. Also Dr. Sumanta Pal of the City of Hope, my own doctor, discusses ongoing use and sequencing of targeted therapies, both from 2013 June ASCO
Delays in being diagnosed with my kidney cancer may have led to it going to my lungs. Bad enough, but I had good care in my treatment–I think. Rarely can a patient analyze his own care for errors. No so with this guest writer, Dr. Itzhak Brook, whose story of his misdiagnosis and numerous treatment errors is one we should read. With rare insight and passion, Dr. Brook is dedicated to prevent medical errors. The following is from his lecture at LSU Health conference in May 8, 2013.
Preventing Medical Errors:
A Physician’s Personal Experience as a Laryngeal Cancer Patient
Dr. Itzhak Brook: Guest Speaker at LSU Health conference in May 8, 2013.
Dr. Brook is introduced: Dr. Brook has written 700 articles. He is an associate editor of several medical journals. He is a member of the editorial board of several medical journals.
I have been very fortunate to serve with him in the “Head and Neck Cancer Alliance National Committee.” That’s where I got to know Dr. Brook, and he is doing some amazing work in terms of lobbying for head and neck patients to get their voice prostheses, electrolarynx, basic functional components that are not covered by healthcare.
Dr. Brook was diagnosed with larynx cancer in 2006. Two years later he had to have a laryngectomy, and he currently speaks with the tracheal esophageal puncture. He is the author of the book, “My Voice: A Physician’s Personal Experience with Throat Cancer.” In fact, this morning he gave our department an inspiring talk on how it is to be a laryngectomy patient, and what we as physicians should look for. Dr. Brooke is the recipient of the 2012 John Connelly Medical Ethics Award by our Academy this year. Once again I would like to welcome him.
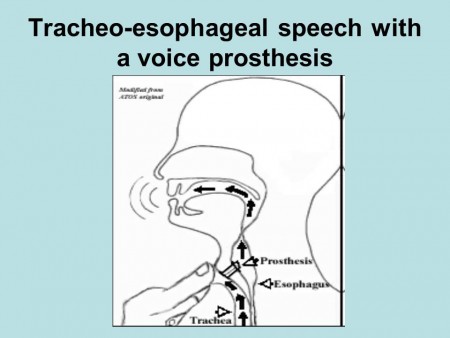
Dr. Brook speaks: “Thank you. It’s a pleasure to be here today and to talk to you about medical errors. First of all, I hope that you can all hear me. I have a very low voice when I speak. I speak with the voice prosthesis. Here is a diagram of how I speak. I do this by diverting air through a little prosthesis into the esophagus and where the air and the vibrations created allow me to speak. This is my challenge: to be able to maintain the seal with this device around my neck which allows me to speak. I wanted to talk to you today about my experiences as a patient with throat cancer and how I encountered many of these errors from nursing, then physicians while I was patient, and how I suggest we can prevent those errors by better education, patient advocacy, and how we can improve patients’ care.
It was shocking to me –when I became a patient to realize how common they are. I have been a physician for more than 40 years, but I had never been on the other side of the stethoscope. As a physician learning on my own the seriousness of those errors, there wasn’t a day in which I did not notice two or three errors that were done by nurses, physicians, technicians, nutritionists.
It was psychological and physical strain to be on the watch all the time to try to prevent errors. I realized that hospitals are very dangerous places to be. Not that I didn’t know it, but this really illustrated how it’s a miracle that patients get out without more damage than they came in with. Indeed in surgery, it’s estimated that about a third of all patients end up with some kind of permanent or temporary damage because of mistakes.
Imagine how lucky that I was the medical professional, that I was able to observe those errors. The layperson is much more susceptible to them and cannot even correct them. Many patients are intimidated and are so grateful to us that they don’t voice their concerns or criticisms. That is why we don’t hear, and we don’t prevent many errors that can be prevented–even when they are observed. People like myself who have difficulties in speaking, especially after surgery when I could not speak for six weeks, are much more susceptible to such errors.
Let me share with you, first of all, what I saw in my own eyes as far as the errors I encountered. The first one that I noticed was that my physicians failed to recognize that my cancer had returned–even though I came to them with complaints of pain. They relied on an imperfect physical and endoscopic examination. They relied on the fact that the CT, MRI and PET scans were all negative.
But there was no substitution for a good physical exam which they neglected to do. What they should have done was asked me to do a Valsalva maneuver while doing an endoscopy, to breathe air and hold it and then look. This allows parts of the upper airway, most specifically the pyriform sinus to open, which reveals an area that is otherwise not seen. My tumor was already an inch long and it was missed by CT, MRI and PET. That was an example that the diagnosis can be made in many cases by good physical exam.
The other thing that I learned is that some of the mistakes were because of the physician’s lack of experience. My surgeons offered me a procedure which they had only done once before. I was desperate to get the cancer out and neglected to think about it myself, as “You need this procedure, but there may be people across the country who have done it hundreds of times.” What they told me is, “In surgery you see one, you do one, and you teach one.” I believed it, but I know it now it should be, “You see 1000, you do 100, and then you teach one.” This is the reality of the world.
As physicians, we like to help our patients, but we should know our limitations, and in fact, that we are not able to be expert in everything. It’s okay to admit it and refer patients to people who know more. Some cancers are so rare, like larynesophageal cancer, thanks to fact that less people smoke and drink, even at the Centers of Excellence, their number is limited. It’s okay to admit that some procedures are better done by those who do them more often. The fact that they removed scar tissue from me instead of the cancer speaks to my surgeon’s inexperience in the technique they used.
Another error I noticed was that my physicians wrote my orders in the wrong chart. Consequently I did not get the right treatment and I got therapy for another patient. This occurred in one of the best medical centers in New York City. You can appreciate that even in the best places mistakes do happen, and these are just a couple of several errors my physicians’ made in my care.
Nursing errors are more common and range from not responding to calls to forgetting to connect the call button to my bed. I was in ICU a day after my laryngectomy, and my bed was only three feet away from the nursing station. I was connected to five different tubes, IV lines, catheters. Suddenly I was choking with secretions. I couldn’t cough them out so I looked for the button to call the nurse. I could not find the button that fell to the floor because it was not attached to the bed appropriately. To save money the same nurse was serving two other ICU patients. My nurse was away. I couldn’t call for help. disconnected my PO2 monitor. Nobody came. I disconnected the EKG monitors. I thought they would see a flat line.
Nobody came. Fortunately, my wife just happened to come in the morning, and she called the nurses to suction me.
Imagine that this can happen in ICU. You can choke to death! Not every hospital has one nurse for three patients. When I was first hospitalized in military hospitals they had one nurse per patient. But in that hospital in New York, they were saving money. So here’s an example of a serious nursing error.
Some of the errors are listed here–like not washing hands, not covering the thermometer with the plastic cover, using the improperly sized blood pressure cuff, leading to alarming results. That meant I got medications to lower my blood pressure which wasn’t high, and administering the wrong dose of medication. So these are some of the mistakes.
There is a lot that can be done to prevent errors when better and uniform methods are used for training.
What is important is to adhere to certain standard of care. The rule now is to use algorithms and check lists. Algorithms have been shown to prevent many errors. Simply by following the chart, you don’t forget about it; reviewing the records to detect errors and to admitting it and training the personnel to prevent it. There are people who keep making mistakes—those individuals should be retrained or even dismissed. They should be reprimanded.
It’s also important to have better supervision and encourage patient advocacy. Encourage patients to talk about those errors. Admit them if you think you made a mistake. Admit it and don’t try to wash it away. Admitting will prevent malpractice suits. Patients who see that the personnel acknowledged their errors will be less likely to seek reparation. If they don’t see it they are more likely to look for punishment.
That is why open discussion is important. Encourage patient advocacy. Tell them the truth. Tell them the treatment plans. Let them be your eyes and ears, so they can come and correct, and tell you if something went wrong. It’s important to ask friends or advocates to help patients make the right choices so that mistakes are not being made. Encourage second or even third opinions. There is nothing demeaning about it. It will also make the patient know that you are there to help them choose the right treatment.
What patients should do is look for the experts in their illness field. Sometimes patients make mistakes by confusing friendliness with expertise. I made those mistakes. My physicians were lovely human beings, but still those that I initially saw did not have the best expertise in my illness field.
Ask for the true prognosis. Don’t be always optimistic, but realistic so if things don’t work right, the patient should know, recognize and accept it. What I tell patients to ask for, and you should also encourage them to do is to give you their best history. The more you know, the easiest to it is to prevent errors. All the past history, all the little nuances that patients can tell will help their doctors make the right choices. Also what I ask the patient to do is to challenge us. Ask questions. Don’t dismiss these questions. We the physicians should not overshadow our patients. Let them ask. They may not always know something. Tell your patients, “Don’t assume that we the doctors know everything because we don’t.”
Medicine is as much an art as it is science. If the patient has an advocate, they are going to be more likely to catch errors and explain and ask questions, especially when the patient is sleepy or sick. Have a friend or family member be there and challenge us if necessary will prevent errors.
All physicians including surgeons need to listen to thire patients. We are all overworked, but we need to recognize how overwhelmed the patient is. They cannot always make good judgments. They are scared. They want to be saved and helped and they don’t always ask the right questions. You need to let them have time to question you, to challenge you. The more explanation you give, the better they will be in helping you prevent mistakes.
Don’t forget to examine the whole patient, not just the area where you specialize in. I especially ask my surgeons to examine on the entire body. I asked my surgeon to listen to my lungs, he said, “I really wouldn’t even know how to do it that. I’ll call the internist.” I was shocked o hear it, but at least he recognized it as his shortcoming.
You need to remember the patient is made up of body and mind. Don’t forget to think about the patient’s psyche as well and the all other issues that are psychological. They all contribute to what we call the whole patient. It’s important to recognize thoseissues and educate the young medical generation, the residents and fellows about those issues. Residents follow us, the attending. If they see us, the attending, to be patient and concerned they’ll do the same. That’s why it’s important to follow those guidelines
It is important to educate the young generation to make sure they develop good treating habits and will care for the patient and will catch errors and be more humane and caring.
I summarized a lot of what I talked about today on my blog which is listed here (http://dribrook.blogspot.com/) where I discuss also medical errors. I have a page on my blog that discusses how to prevent medical errors and what were my own experiences. This is a difficult, and a challenging topic. We can prevent many of those errors by encouraging better adherence to standards of care, patience, vigilance and advocacy. By preventing making mistakes we will get better results and better patients satisfaction.
I want to thank you for your attention. I will be happy to answer your questions. Thank you.”
Questions from the audience:
Audience; “One of my observations and thank you for presenting. My observation is that one of the major problems with medical errors is that most people don’t care or they think it is someone else’s responsibility. We don’t recognize our responsibility. Something else to the younger generation: they need to they need to feel confident enough that they will allow patients or advocates to challenge us. There are many physicians who are either overly self-righteous or afraid that when they’re challenged, their entire being has been challenged. They don’t feel comfortable enough to have a discussion like that with the patient or advocate.”
Brooks: “You are correct. Many physicians are threatened. Many come in today with the Internet more knowledgeable. Many patients know a lot about their illnesses and the more I think: the more they know, it is better. On the other hand, there is lot of false information that the patients have through many sources of knowledge that are not perfect. I think that we should encourage it. I don’t think we should see that as a threat to us. Get patients, let patients challenge us.
I can tell you that as patient I was afraid to challenge my doctors. I was so grateful initially that they were taking care of me, that I was afraid that if I would challenge them, they wouldn’t give me the best treatment. It may sound strange, but I was afraid. I was afraid that they will label me a troublemaker. So I kept silent. I was silent anyhow, but at least I didn’t say anything in writing. As the mistakes accumulated, I realized that “If I don’t speak out, I will not get out of this place as healthy as I could”, and I started to speak out. My luck was that my daughter was my voice for a while, until she had to leave. She was my patient advocate.
But many patients are threatened by us even if we are nonthreatening. But we can try to disarm them and create an atmosphere of less threat and can encourage them to talk instead of being defensive. We would say okay, let me look into it and let me do something to about it.
One of the most humiliating episodes that happened to me occurred when I was recovering from my laryngectomy. That one morning the residents were making rounds. I had a laryngectomy tube—which was completely clogged with mucus. The nurse usually came and cleaned it, but she hadn’t yet. The residents got there first. So I asked a resident to clean it. I was shocked when he took it out without gloves, went to the faucet and flushed it with water. I refused to let him put it back in my trachea – in my tracheostomy. I wrote to him, “This is not the way you should clean it. You need to open a kit and do it.”
He said to me, “We are running the show now. This is how we do it.”
I was so helpless I couldn’t do anything except refuse him from doing it. When I mentioned it to the attending (physician) when he came, he told me “Oh, this is resident is very nice. He would never behave like this. I can’t believe he did it.”
I didn’t hear anything more about it. So there was an example of the mistake. You don’t clean it with tap water! You have a kit. You need to wear gloves. This is also an example of arrogance. There is no room for arrogance.
Now if I was in a position to do it, if I could walk, I would go to the hospital director and complain but I was a sick, helpless patient. Here is an example of how a patient can’t do anything. He is completely at the mercy of staff and mistakes that are being made. So I think there is a need to better education, for greater humility, and less intimidation.
Also there are places where the nurses are not as well trained. I noticed a difference in the quality of nursing. When I was hospitalized at the Naval Medical Center in Bethesda I noticed that the nurses were young but very well-trained. Everything was done according to the book. However, when I was hospitalized at Walter Reed Army Hospital, I found out that about two thirds of the nurses were civilians, from many places. Some were good, but some were not. Some nurses were well-trained and some were not. You need to make sure that everybody is following the same procedure and that is best way to prevent mistakes.
Audience: “I think you need to go around the whole country to teach us about this. This is the tip of the iceberg. You are a physician, you are an insider, you know what happens there so you can say I have a job I don’t do much. The problem is the education that you mention. To be critical, you have to suffer pain. People like to be praised all the time, “You are doing a good job, you are doing a good job.” If one harms you, say at this time that it is wrong, so the next time you praise will be appreciated. You’re coming from a high school, a college, medical school and something and so, and told. “Be nice, not to be critical” We are not critical enough. The problem is big!”
Dr. Brook: “I couldn’t agree with you more. It’s important. At one point I said enough, I guess I’m not going to be a nice guy anymore. I am going to take the gloves off. I am extremely grateful to everybody and I say it to them. But on the other hand, I realized that we are all human beings. We all make mistakes. It’s not a perfect world and the only way we can prevent it, reduce it, is to have check lists. We need a system that reduces it. One thing is to have lesser burden on the physician, lesser burden on the nurses, so that they are not overwhelmed, so that they don’t make mistakes because they are tired and overworked.
We should have a system where people are encouraged to admit and discuss mistakes openly so we don’t repeat it. We have in our own hospital such a venue where we meet once a month and we talk about the mistakes we made–without accusing anybody, without reprimands, just to talk, to prevent the errors from happening again.”
Audience: “We have to listen to what you are saying…The part I found most important for young doctors, that we have to emphasize over and over again is the importance of a good history and a good physical exam. Some of our younger doctors think that a physical exam is complementary to the technology and it should be the other way. Technology should be complementary to the physical exam. We are missing a lot and need to go back and listen again sometimes you have to remind yourself that just because we have CT scans and PET scans, it’s not the same as talking and having the doctor patient relationship .
Dr. Brook: “I agree that we forgot the art of medicine over the years. I remember when I went to medical school in the 60s, how my teachers were really true clinicians. They could examine the patient and listen to them and talk to them and they were able to find things. Today people forgot the art of medicine. I believe that even today 95% of the diagnosis can be made by doing a good physical examination. Unfortunately the new technology made us rely on tests and scans and in this way we spend less time with the patient and that course also leads to mistakes.”
Audience: “The question I have for you is with cost being such an issue now, I think, what are we to do with less staff when there’s still a need for extra eyes?”
Brook: “I think there is no substitute for more staff. When someone is out of surgery in the ICU and in critical condition, you need a person there. I don’t think there is a substitute for that. I wrote about those episodes in my book. There was an episode when I was mistreated because of lack of personal. I had a skin flap removed from my hand to create my new esophagus. That flap needed to be constantly covered. The nurse was in the process of changing the cover when she had to suddenly leave my room because she had something else to do. I was lying there for about 20 minutes. I couldn’t call anybody. When I finally got somebody, they told me, “The nurse is on the phone ordering something.” A resident physician who came to complete the change was called away by the attending. Nobody seemed to care that I had tremendous pain for another 25 minutes. There is simply sometimes pure negligence that happens. The only thing I can tell you is that a patient advocate is so much needed. I know that if, God forbid, anybody of my family will be in the hospital, I will not leave their side 24 hours a day. Fortunately, it didn’t happen to me yet but if it will, I will not leave their side.”
Audience: “What I think this episode reveals is simply what Dr. Mary says, that there is a loss of professionalism amongst everybody involved in healthcare. There the physicians, I think have forgotten that they’re in charge of everything. We do need to hold everyone accountable. The nurses have forgotten what their true training has been in. Everybody has focused on getting the work done as quickly as possible so they can get onto the next thing. It has left the medical profession in the dark.”
Dr. Brook: “I agree with you. People are so overwhelmed. Sometimes when I wanted to talk to a physician (by writing because I couldn’t speak) he would dismiss me, “I’m really very busy now, I have to run to my clinic or I have to run to the OR. If you like, have your wife call me.”
I had one mistake that happened because the doctors wrote an order for another patient in my chart–to start feeding me one week after the surgery. It seemed to me very strange, because I remembered that my surgeon told me that I will be starting feeding two weeks after the surgery. I protested, but then I thought, “Maybe it is all right. I’m happy to eat again”. Only because I questioned it again and again, did they finally stop it–twelve hours later when they realized they made a mistake. I was fortunate that no bad thing happened because of it even though after getting the type of surgery I had, it was dangerous to be eating too soon. Here is an example of an error and I don’t even know if there were any repercussions because of it!
I wanted to let you know that you that you could read my book, “My Voice: A Physician’s Personal Experience with Throat Cancer”. It’s available for free on the Internet at my blog and also you can get it from the American Academy of Otolaryngology website ebooks site at http://www.entnet.org/mktplace/ebooks.cfm
I love this study, as it really symbolizes the tremendous change that has occurred in kidney cancer treatment these last 6 years. It is remarkable that the 124 patients are described as having already received first- line treatment, and were now in their second-line. These same metastatic patients might have received neither just six years ago.
The study was really not to compare the response to the treatments received, whether Sutent (sunitinib), Nexavar (sorafanib), or placebo. (Why any party chose or was chosen to receive a placebo is another, darker question.) That the median follow-up was 80 months is a triumph by itself. This is in contrast to the clinical trials that often show just a few months extra time which we and politicians can focus on, when the reality of much longer responses is clearly shown here. Of course, these longer survival times came from those trials which showed those few months–and this shows the reality of many more months and years of life!
Metastatic tumor burden(TB) was measured, based on the size of the sum of the longest unidimensional diameter of each targeted lesion. The additional increase of 1 cm (about 3/8”) was significant in predicting response to the medications. Siimply, adding the one-direction measure of the lesions and comparing them showed that more tumor was a bigger problem.
One can also assume that to remove as much tumor as possible may be helpful in maximizing the benefit of the meds given, although this study does not address the actual types and locations of the mets, nor indicate why no other therapies, surgery or ablation, were used. With 124 patients this would represent a mix of individual experiences, more like the typical patient group.
What does “median follow up of 80 months” really mean? A median is not an average, but a measure of the time point at which ½ of the population studied had follow up less than 80 months and ½ had follow up for more than 80 months. Since this is considered a long time in clinical trials and becomes more of a longitudinal study, we may never know the average length of time that these patients had either PFS (Progression Free Survival—time until the mets began to grow again) or OS (Overall Survival). In any case, we are aware that following this second-line of treatment, there are still more therapies and interventions which may be available. And even more options are up for FDA approval as I write.
All these options and the greater success of each muddies the study waters, but clarifies the hopes of those with metastatic RCC, or are at risk. This study proves that tumor burden (TB) is a disadvantage. Most patients have naturally assume that more cancer is worse for you than less cancer—who knew? But this gives weight to the notion that the removal of some tumors, if not all, can be beneficial used with targeted therapies. In the past, some oncologists have discouraged additional surgery in the light of metastases, with the implicit message, “It’s too late, and won’t help you anyway.” Not the doctor for me.
The story is quite different right now, but patients may need to tell this to their doctors–in the language that the doctor speaks. Certainly, there was a time at which doing more surgery for mRCC patients added little, if anything, to survival and probably even less to the quality of life. That no longer is the case, and those older studies no longer have meaning. While each patient must be treated as an individual, in light of all the variables that impact his health, there is increased optimism for the metastatic patient. Aggressive and early treatment can no doubt extend life and make it worth living.
Halfway through my high dose interleukin 2 (Proleukin) treatments, having completed weeks 1 and 2 and into the second rest period, I got the second most important scan of my life. The most important CT scan changed my life, with its image of a tumor larger than a baseball, and countless tiny specs of white death in my lungs.
This new scan in August of 2004 would let me return to the hospital for more of the immune stimulant, Proleukin, which revved up my internal immune system to the max. My system was then to recognize and fight off the residual kidney cancer that had settled visibly in my lungs and any other new sites, as yet unseen. The new vocabulary of cancer forces me to say that while hundreds of tiny lung mets/lesions/nodules–no wonder we patients get confused–were not just there, but ” visible”. Implicit was the message that many hundreds more were invisible, certainly alive and thriving, just not yet “imaged”.
The tools of imaging cancer are varied and unequal, some more effective for some cancers, and yet inadequate for others. First of all, the tumors are measured in centimeters and millimeters, and that language shift alone makes them even more inaccessible to Americans. Just how big is 9 millimeters anyway? And a centimeter seems a pretty vague measurement after years of holding thumb and forefinger together to how 1/2 inch with decent precision. Is a change from7mm to 9mm cause for alarm?
Plus the panic of hearing “cancer” drives any math computation out of one’s head. The only math question that can be asked and then not understood is, “How long have I got, doctor?”. And then there is the matter of what can be seen with which instrument. When doctors tell smokers that their x rays are clear, naive civilians translate that to mean their lungs are free of cancer. A rough interpretation might be more like, “Your tumors–if you have them–aren’t big enough to be captured by this 100 year old device. Come back when we can see something/you are pretty much past help.” Notice that I provide the translation here.
The x ray is more like using a child’s microscope to look at something; great for noticing crud on your pet’s hair, but not quite like those grownup electron microscopes which can see cells. Note to kidney cancer patients–don’t even bother.
Another imaging device is a PET scan, which measures the activity of cells, and which I understand a quick snap shot of liveliness of the cell, and it manifestation, the tumor. Is it chowing down on the body’s nutrients faster than the orderly cells? That activity will “light up” in a PET scan, so the lazier cancer cells might be overlooked. Not to effective in kidney cancer, whose tumors are often slow-growing. That is also possibly why kidney cancer can establish itself so thoroughly in so many patients, not noticed until a broken rib or vague back ache or a non-existent ulcer finally results in a CT scan. Note to lots of kidney cancer patients–don’t even bother with a PET scan.
So a CT scan, with contrast to enhance the vague and ghosty images is the way to go for most RCC patients. A blood test to see if the single kidney can handle the assault of the imaging fluid precedes the test, and then the patient settles onto a big padded tray which is drawn slowly into a large doughnut-shape machine that somehow can see into the patients insides. I’m not even trying to explain that.
That exam is not painful, not pleasant, and not anything you can study for; you simply submit, as patients are supposed to do, and then the impatience begins. Most patients must wait to get their results from the doctor, and this is the longest wait of one’s life. Am I dying more efficiently than before? Are the cells multiplying more quickly? How long have I got, doctor?
But I had learned the secret, which I now announce to all. You are ENTITLED to your own reports, and with a bit of research as to when they get read, you can go get them. Apparently for many imaging centers, this comes as a surprise, but we are all grownups and can explain that. Sometimes your doctor will need to hear that too. I have always just called ahead to the “Medical Records” department and asked for the report to be ready, as I have no patience…again.
But in August 2004, I had to be outside before I could read it. To read a report of impending death inside a hospital with its metal window frames and linoleum floors and sad, bent people waiting their turns is too harsh a setting. Immediately stepping outside, I could rip open the envelope, and read that my lung tumors were shrinking, even those big ones. The 13mm lesion was now 8x9mm, the 8x7mm lesion was just 4x4mm. And the countless other unmeasured one? They were likely shrinking, too. And 9mm is .354 inches, which I still can’t measure between my thumb and forefinger, but the CT scan could, and that was good enough for me.
Back to the hospital, a much easier trip than before, to get two more week-long sessions of HD IL2. The mets were shrinking and I was getting more ammo against them. The cloak of invisibility was pierced and my immune system was working again.
My first week at home following the CT scan was to be a recovery week, following five days in the hospital. When I had anticipated that first weekend, post Proleukin/High Dose InterLeukin 2 treatment, my plan was to go to a local kidney cancer meeting. I would be a bit soggy, post “flu”, but not contagious, just recovering from the immune stimulant. I planned to sit around, smile bravely, and look like those heroines in the old days of consumption.
As a measure of my mental competence, it was several weeks later before I realized I had missed the meeting, and in fact, had missed most of the week, and a good portion of the recovery week as well. My response to the Proleukin was such that I did not receive but 9 of maximum 14 doses and had to spend an extra day in the hospital to recover. The last thing I do remember of that week at UCLA was a doctor walking me down the hall, and seeing a sign overhead. At least I could read, and knew I was in the hospital, and then somehow I was home.
Flashes of memory come to me of those first few days, retching in the toilet, and then being sat in the shower on a tiny plastic stool, and being scrubbed by my daughter, a miracle of an experience. And more odd oblivion. At this time, my mother-in-law was headed deeper into an oblivion of Alzheimer’s, and I joined her. One WEDNESDAY morning, I was reading the paper v e r y s l o w l y…not my usual style, and I noted that the LA Times used Tuesday’s date. Obviously this was major mistake, which rather incensed me, and tried to interest my husband in this crisis. “What day is it?” He also thought it was Tuesday! For that matter so did the local paper, and the Wall Street Journal!
Naturally, I had misread or misheard this, so checked again, and asked again, and asked again, and read again. Even the damn computer was in on this mistake, but I waited patiently for corrections to occur, and still they–now the entire world–claimed it was Tuesday. And the family was getting a little odd in their responses to me. “Still Tuesday, Mom…”.
Not once all that Wednesday nor the Wednesday that followed it did I ever think for a second that I might have been mistaken. My testing, my logic, my checking and rechecking all these reliable resources did not change my mind, but it did cause me to wonder why everyone else was wrong. I figured the nice thing to do was to wait until they got it right.
It took me several months and a number of similar events to realize that this was a tiny gift from HD IL2–and insight into craziness, or whatever word describes the inability to accept fact in the face of facts from trusted and even beloved sources. No wonder poor Nana could get so angry at all of us, and no wonder that telling her something in a logical manner was futile. Her brain had been compromised by Alzheimer’s and mine by the medication that was trying to save the rest of me.
So was it working? Brain issues aside, I felt fine, or so I told my oddly polite and amused family. Taking a plate to the sink proved to me that I was doing all my household duties. Writing a 25 word email in 30 minutes proved my computer skills were intact. But what about those precious lungs and the icy white granules of tumor dividing relentlessly?
Without proof that the IL2 treatment was slowing down the growth, I would not have been permitted back into UCLA. To push the immune system into the kind of response that causes it to seek and destroy the cancer cells so well-settled into my lung, not only the visible ones, but their countless and invisible spores, is dangerous. No doctor wants to make a patient sick without hope that this synthetically induced sickness would drive out the virulent and relentless cancer cells, so it had to be shown to be worth the risk.
As I really became aware that I had missed one week and more in my life due to the treatment, and that I had no control of memory over what had happened in the hospital, I realized how hard it would be to readmit myself to the hospital. Excuse after excuse–all good ones, of course–delayed my walk into the lobby, accompanied for the first time by fear.
Years earlier, as my father lay dying in our family room, he told me that he was afraid to go to sleep, for feared he would wake up dead. We grinned wryly, and promised not to let that happen, though it did–everything but the waking up. I was raising my hand and volunteering to do just that, walking back in through the gray and damp parking entrance to UCLA.
Coming out the second week with equal blank spaces and some low blood pressure “events”, I was still alive, and could plan for my CT scan. Back to the same place where they had first found and failed to tell me of the lung mets, and let them try again to “image” them. (Is image now officially a verb?) One thing remained in my brain, and that was the knowledge of how to get the report from the CT scan done two weeks plus into my rest period after week two.
My son drove me to the scan center, as I was oddly not thought to be capable of going there myself, such a smart family, and parked as I rushed to collect the report. It was at the desk, as promised, and I tore open the envelope, and pulled up the last few sentences of the report into view. “Significant decrease in size of multiple pulmonary nodules!”
And back for more Proleukin. And a cake that I ordered for myself, which read (Charlotte’s Web alert) “Zuckerman’s Famous Peg…Amazing.”
Every family who encounters cancer has a struggle, but nothing seems harder to bear than the stories of those who are hit when they are especially vulnerable. When I was diagnosed, my youngest was barely 17, but the others were grown and independent. When cancer hit this family, they had a newborn. Against all odds, this a success story, and one which reminds us of the value of love and strength. I introduce the story of Cameron Von St James and his wife Heather, in this guest post:
“More than once, my wife has made the comment to me that she doesn’t know how I coped when she was diagnosed with cancer. Her mesothelioma diagnosis came only three months after she gave birth to our daughter Lily. What was a joyful, happy time in our lives turned quickly into a time filled with fear and uncertainty. When Heather’s doctor told her about her cancer, I looked at her, and she broke down crying. I didn’t know how we would get through this.
I was so overwhelmed with emotion. I was on the verge of breaking down when the doctor’s words brought me back to reality. He was talking about making medical decisions for my wife, and I knew this was just the beginning. It was the first of many days where we would be forced to make impossible decisions while going through overwhelming emotional turmoil.
My overwhelming emotions didn’t stop there, however. Following her diagnosis, I was angry at the world. I felt like it wasn’t fair that we had to go through this. For a while, I often lost control and lashed out at others. I used a lot using profane language. It didn’t take me long to realize how selfish I was being. The last thing my wife needed was to see just how scared I really was. I knew I needed to get it together and be strong for Heather, but it was so hard for me to do. When I was able to do it, I finally became the rock that she needed.
I was still overwhelmed with the new responsibilities that fell on me. I had a mile-long to-do list that included everything from travel arrangements to work to taking care of my house and family. I wouldn’t have been able to get through any of it without the help offered by our family and friends. I learned to prioritize and to first get done the things that were most important. I was still overwhelmed even with all the help, but I managed to get through it.
The hardest part of it all was sending Lily and Heather to South Dakota for two months following Heather’s surgery in Boston. I knew that I couldn’t work and take care of Heather while she recovered, and that’s what forced us to make this difficult decision. Heather’s parents in South Dakota offered to take care of them while Heather recovered and prepared for the next round of her mesothelioma treatment, and we decided to accept the offer. During that two-month period, I saw my family only once. I left work on a Friday night and drove 11 hours in a snowstorm to see them. I had to make the 11-hour drive home that Sunday so that I could be back at work on Monday morning.
What I learned through all of this is how lucky we were to even have difficult decisions to make. I was so lucky to have the help I had from all of our friends and family. I couldn’t have done half of what I did during this difficult time without their help. You have to accept help when it is offered to you during times this difficult. It’s been six years since Heather was diagnosed, and despite the overwhelming odds against her, she’s happy and healthy now, and cancer-free. I only hope that my words can help someone else who is going through cancer.”
Is there a difference? How do I choose? Do I get fries with that?
I need CT scans of my chest, pelvis and abdomen, or at least I did. Eight years ago, I was diagnosed with Stage IV cancer, got healthy, but still need pre-emptive CT scans.
Metastases were all over my lungs, and the kidney dug out of my belly, so I get “CT scans of the chest, pelvis and abdomen, with and without contrast. Compare to previous scans.”
Consistency of scans is important, so I am scanned at the same place, prepped by the same nurses, and have reports from the same radiologists. Only billing is inconsistent.
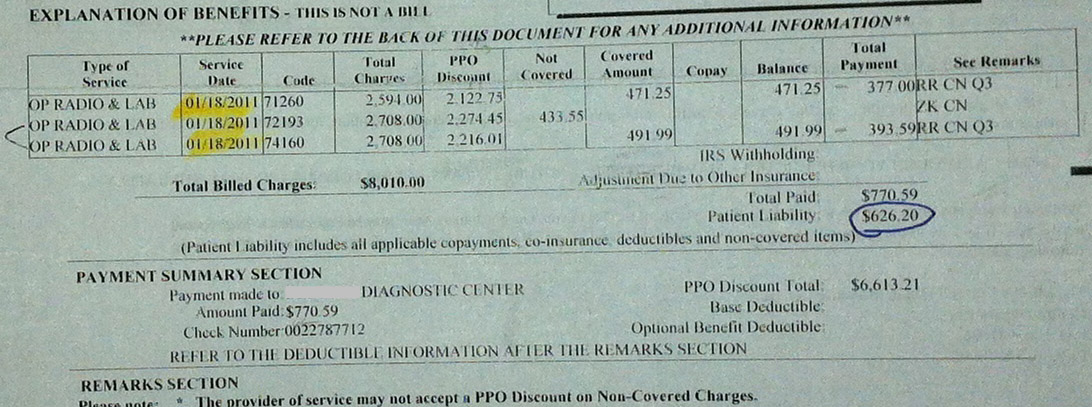
My EOB showed three scans, three CPT codes, three “retail” prices, totaling $8010, and three insurance prices discounted by $6613. Good so far.
Insurance pays their portion, less some amount, giving the provider $770. I am billed the balance of $626, worth $1396 to the provider.
Before my next appointment, Medicare decided that pelvis and abdomen scans done simultaneously are one procedure. Unsure where the abdomen ends and pelvis begins, and where the kidney fits, and how low the lungs go, this made sense. It did not affect my scans nor my report.
As the three CPT codes became two, (72191 +74160= 74177) the beloved discounts didn’t accompany those codes. With the $1000 maximum daily payout by the insurance company, my $8010 scans were calculated to charge me $4074! Now the scan was worth $5074?
Not happy, and not about to pay, I asked the cash price of the scans. Just $930!
Calls to the insurance company, the third party whomever, the billing department and trips to the billing office, and subsequent calls to the state insurance office. And the letters to the collection company and the whining…
My best offers were “charitable assistance, paying the bill over two years”, and “just tell Medicare to change the codes back”. That I offered to pay my fair share and that I wasn’t a Medicare patient meant nothing. And have you ever “just told” Medicare anything?
Time for another scan: “I’ll take the cash triple CT”, and asked to be billed directly. The $930 scan was a bargain after the days spent fighting for my $626 scans.
Murphy’s Law applied, so my insurance was billed, not me. Thus, another $4074 bill to me. And the trips and calls started again.
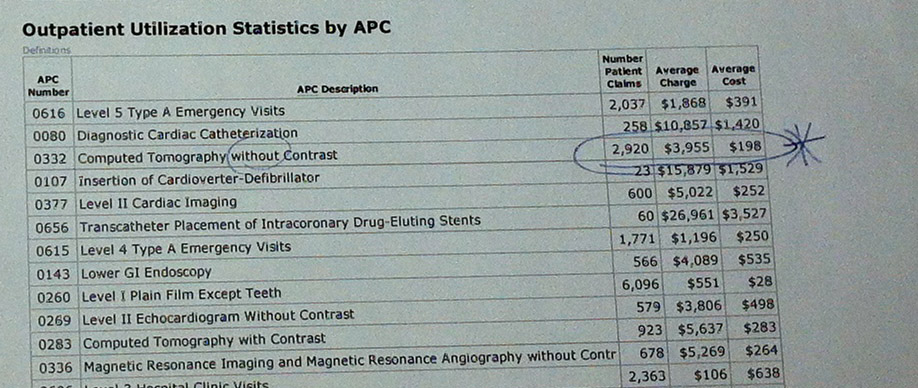
What does the typical CT scan really cost, per the hospital’s published reports to the American Hospital Directory? My provider states a single “CT without Contrast” to be $198, but $60 at their satellite center. With contrast, the figures go to $283 and $89, respectively. Assuming I get three of the $283 scans, it costs $849—close to the cash price. Maybe I should get my scans from the satellite center at $89 x 3, for $267, really a deal!
No wonder there is such anger and distrust with the medical system, and not only with the insurance companies. The providers play the same game with the payer—whether the individual, Medicare or Medicaid, or an insurance company. The least empowered figure is naturally the individual, but in the long run, the anger and the cynicism generated drives a wedge between the patient and his individual providers.
The doctor who prescribes a CT scan and its cost has no idea—even the provider has no idea. And who is most vulnerable, and most likely to put off the scan? Me. And you.

 Me,
Me,