
Delays in being diagnosed with my kidney cancer may have led to it going to my lungs. Bad enough, but I had good care in my treatment–I think. Rarely can a patient analyze his own care for errors. No so with this guest writer, Dr. Itzhak Brook, whose story of his misdiagnosis and numerous treatment errors is one we should read. With rare insight and passion, Dr. Brook is dedicated to prevent medical errors. The following is from his lecture at LSU Health conference in May 8, 2013.
Preventing Medical Errors:
A Physician’s Personal Experience as a Laryngeal Cancer Patient
Dr. Itzhak Brook: Guest Speaker at LSU Health conference in May 8, 2013.
Dr. Brook is introduced: Dr. Brook has written 700 articles. He is an associate editor of several medical journals. He is a member of the editorial board of several medical journals.
I have been very fortunate to serve with him in the “Head and Neck Cancer Alliance National Committee.” That’s where I got to know Dr. Brook, and he is doing some amazing work in terms of lobbying for head and neck patients to get their voice prostheses, electrolarynx, basic functional components that are not covered by healthcare.
Dr. Brook was diagnosed with larynx cancer in 2006. Two years later he had to have a laryngectomy, and he currently speaks with the tracheal esophageal puncture. He is the author of the book, “My Voice: A Physician’s Personal Experience with Throat Cancer.” In fact, this morning he gave our department an inspiring talk on how it is to be a laryngectomy patient, and what we as physicians should look for. Dr. Brooke is the recipient of the 2012 John Connelly Medical Ethics Award by our Academy this year. Once again I would like to welcome him.
Dr. Brook speaks: “Thank you. It’s a pleasure to be here today and to talk to you about medical errors. First of all, I hope that you can all hear me. I have a very low voice when I speak. I speak with the voice prosthesis. Here is a diagram of how I speak. I do this by diverting air through a little prosthesis into the esophagus and where the air and the vibrations created allow me to speak.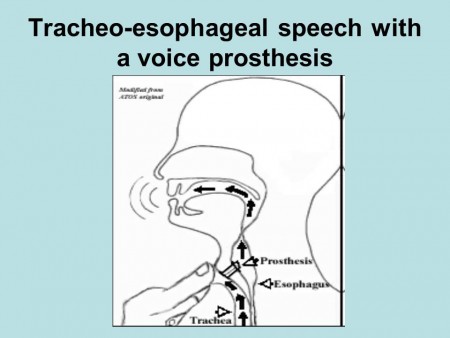 This is my challenge: to be able to maintain the seal with this device around my neck which allows me to speak. I wanted to talk to you today about my experiences as a patient with throat cancer and how I encountered many of these errors from nursing, then physicians while I was patient, and how I suggest we can prevent those errors by better education, patient advocacy, and how we can improve patients’ care.
This is my challenge: to be able to maintain the seal with this device around my neck which allows me to speak. I wanted to talk to you today about my experiences as a patient with throat cancer and how I encountered many of these errors from nursing, then physicians while I was patient, and how I suggest we can prevent those errors by better education, patient advocacy, and how we can improve patients’ care.
It was shocking to me –when I became a patient to realize how common they are. I have been a physician for more than 40 years, but I had never been on the other side of the stethoscope. As a physician learning on my own the seriousness of those errors, there wasn’t a day in which I did not notice two or three errors that were done by nurses, physicians, technicians, nutritionists.
It was psychological and physical strain to be on the watch all the time to try to prevent errors. I realized that hospitals are very dangerous places to be. Not that I didn’t know it, but this really illustrated how it’s a miracle that patients get out without more damage than they came in with. Indeed in surgery, it’s estimated that about a third of all patients end up with some kind of permanent or temporary damage because of mistakes.
Imagine how lucky that I was the medical professional, that I was able to observe those errors. The layperson is much more susceptible to them and cannot even correct them. Many patients are intimidated and are so grateful to us that they don’t voice their concerns or criticisms. That is why we don’t hear, and we don’t prevent many errors that can be prevented–even when they are observed. People like myself who have difficulties in speaking, especially after surgery when I could not speak for six weeks, are much more susceptible to such errors.
 Let me share with you, first of all, what I saw in my own eyes as far as the errors I encountered. The first one that I noticed was that my physicians failed to recognize that my cancer had returned–even though I came to them with complaints of pain. They relied on an imperfect physical and endoscopic examination. They relied on the fact that the CT, MRI and PET scans were all negative.
Let me share with you, first of all, what I saw in my own eyes as far as the errors I encountered. The first one that I noticed was that my physicians failed to recognize that my cancer had returned–even though I came to them with complaints of pain. They relied on an imperfect physical and endoscopic examination. They relied on the fact that the CT, MRI and PET scans were all negative.
But there was no substitution for a good physical exam which they neglected to do. What they should have done was asked me to do a Valsalva maneuver while doing an endoscopy, to breathe air and hold it and then look. This allows parts of the upper airway, most specifically the pyriform sinus to open, which reveals an area that is otherwise not seen. My tumor was already an inch long and it was missed by CT, MRI and PET. That was an example that the diagnosis can be made in many cases by good physical exam.
The other thing that I learned is that some of the mistakes were because of the physician’s lack of experience. My surgeons offered me a procedure which they had only done once before. I was desperate to get the cancer out and neglected to think about it myself, as “You need this procedure, but there may be people across the country who have done it hundreds of times.” What they told me is, “In surgery you see one, you do one, and you teach one.” I believed it, but I know it now it should be, “You see 1000, you do 100, and then you teach one.” This is the reality of the world.
As physicians, we like to help our patients, but we should know our limitations, and in fact, that we are not able to be expert in everything. It’s okay to admit it and refer patients to people who know more. Some cancers are so rare, like larynesophageal cancer, thanks to fact that less people smoke and drink, even at the Centers of Excellence, their number is limited. It’s okay to admit that some procedures are better done by those who do them more often. The fact that they removed scar tissue from me instead of the cancer speaks to my surgeon’s inexperience in the technique they used.
Another error I noticed was that my physicians wrote my orders in the wrong chart. Consequently I did not get the right treatment and I got therapy for another patient. This occurred in one of the best medical centers in New York City. You can appreciate that even in the best places mistakes do happen, and these are just a couple of several errors my physicians’ made in my care.

Nursing errors are more common and range from not responding to calls to forgetting to connect the call button to my bed. I was in ICU a day after my laryngectomy, and my bed was only three feet away from the nursing station. I was connected to five different tubes, IV lines, catheters. Suddenly I was choking with secretions. I couldn’t cough them out so I looked for the button to call the nurse. I could not find the button that fell to the floor because it was not attached to the bed appropriately. To save money the same nurse was serving two other ICU patients. My nurse was away. I couldn’t call for help. disconnected my PO2 monitor. Nobody came. I disconnected the EKG monitors. I thought they would see a flat line.
Nobody came. Fortunately, my wife just happened to come in the morning, and she called the nurses to suction me.
Imagine that this can happen in ICU. You can choke to death! Not every hospital has one nurse for three patients. When I was first hospitalized in military hospitals they had one nurse per patient. But in that hospital in New York, they were saving money. So here’s an example of a serious nursing error.
 Some of the errors are listed here–like not washing hands, not covering the thermometer with the plastic cover, using the improperly sized blood pressure cuff, leading to alarming results. That meant I got medications to lower my blood pressure which wasn’t high, and administering the wrong dose of medication. So these are some of the mistakes.
Some of the errors are listed here–like not washing hands, not covering the thermometer with the plastic cover, using the improperly sized blood pressure cuff, leading to alarming results. That meant I got medications to lower my blood pressure which wasn’t high, and administering the wrong dose of medication. So these are some of the mistakes.
There is a lot that can be done to prevent errors when better and uniform methods are used for training. 
What is important is to adhere to certain standard of care. The rule now is to use algorithms and check lists. Algorithms have been shown to prevent many errors. Simply by following the chart, you don’t forget about it; reviewing the records to detect errors and to admitting it and training the personnel to prevent it. There are people who keep making mistakes—those individuals should be retrained or even dismissed. They should be reprimanded.
It’s also important to have better supervision and encourage patient advocacy. Encourage patients to talk about those errors. Admit them if you think you made a mistake. Admit it and don’t try to wash it away. Admitting will prevent malpractice suits. Patients who see that the personnel acknowledged their errors will be less likely to seek reparation. If they don’t see it they are more likely to look for punishment.
 That is why open discussion is important. Encourage patient advocacy. Tell them the truth. Tell them the treatment plans. Let them be your eyes and ears, so they can come and correct, and tell you if something went wrong. It’s important to ask friends or advocates to help patients make the right choices so that mistakes are not being made. Encourage second or even third opinions. There is nothing demeaning about it. It will also make the patient know that you are there to help them choose the right treatment.
That is why open discussion is important. Encourage patient advocacy. Tell them the truth. Tell them the treatment plans. Let them be your eyes and ears, so they can come and correct, and tell you if something went wrong. It’s important to ask friends or advocates to help patients make the right choices so that mistakes are not being made. Encourage second or even third opinions. There is nothing demeaning about it. It will also make the patient know that you are there to help them choose the right treatment.
 What patients should do is look for the experts in their illness field. Sometimes patients make mistakes by confusing friendliness with expertise. I made those mistakes. My physicians were lovely human beings, but still those that I initially saw did not have the best expertise in my illness field.
What patients should do is look for the experts in their illness field. Sometimes patients make mistakes by confusing friendliness with expertise. I made those mistakes. My physicians were lovely human beings, but still those that I initially saw did not have the best expertise in my illness field.
Ask for the true prognosis. Don’t be always optimistic, but realistic so if things don’t work right, the patient should know, recognize and accept it. What I tell patients to ask for, and you should also encourage them to do is to give you their best history. The more you know, the easiest to it is to prevent errors. All the past history, all the little nuances that patients can tell will help their doctors make the right choices. Also what I ask the patient to do is to challenge us. Ask questions. Don’t dismiss these questions. We the physicians should not overshadow our patients. Let them ask. They may not always know something. Tell your patients, “Don’t assume that we the doctors know everything because we don’t.”
Medicine is as much an art as it is science. If the patient has an advocate, they are going to be more likely to catch errors and explain and ask questions, especially when the patient is sleepy or sick. Have a friend or family member be there and challenge us if necessary will prevent errors.
All physicians including surgeons need to listen to thire patients. We are all overworked, but we need to recognize how overwhelmed the patient is. They cannot always make good judgments. They are scared. They want to be saved and helped and they don’t always ask the right questions. You need to let them have time to question you, to challenge you. The more explanation you give, the better they will be in helping you prevent mistakes.
Don’t forget to examine the whole patient, not just the area where you specialize in. I especially ask my surgeons to examine on the entire body. I asked my surgeon to listen to my lungs, he said, “I really wouldn’t even know how to do it that. I’ll call the internist.” I was shocked o hear it, but at least he recognized it as his shortcoming.
You need to remember the patient is made up of body and mind. Don’t forget to think about the patient’s psyche as well and the all other issues that are psychological. They all contribute to what we call the whole patient. It’s important to recognize thoseissues and educate the young medical generation, the residents and fellows about those issues. Residents follow us, the attending. If they see us, the attending, to be patient and concerned they’ll do the same. That’s why it’s important to follow those guidelines
It is important to educate the young generation to make sure they develop good treating habits and will care for the patient and will catch errors and be more humane and caring.
I summarized a lot of what I talked about today on my blog which is listed here (http://dribrook.blogspot.com/) where I discuss also medical errors. I have a page on my blog that discusses how to prevent medical errors and what were my own experiences. This is a difficult, and a challenging topic. We can prevent many of those errors by encouraging better adherence to standards of care, patience, vigilance and advocacy. By preventing making mistakes we will get better results and better patients satisfaction.
I want to thank you for your attention. I will be happy to answer your questions. Thank you.”
Questions from the audience:
Audience; “One of my observations and thank you for presenting. My observation is that one of the major problems with medical errors is that most people don’t care or they think it is someone else’s responsibility. We don’t recognize our responsibility. Something else to the younger generation: they need to they need to feel confident enough that they will allow patients or advocates to challenge us. There are many physicians who are either overly self-righteous or afraid that when they’re challenged, their entire being has been challenged. They don’t feel comfortable enough to have a discussion like that with the patient or advocate.”
Brooks: “You are correct. Many physicians are threatened. Many come in today with the Internet more knowledgeable. Many patients know a lot about their illnesses and the more I think: the more they know, it is better. On the other hand, there is lot of false information that the patients have through many sources of knowledge that are not perfect. I think that we should encourage it. I don’t think we should see that as a threat to us. Get patients, let patients challenge us.
I can tell you that as patient I was afraid to challenge my doctors. I was so grateful initially that they were taking care of me, that I was afraid that if I would challenge them, they wouldn’t give me the best treatment. It may sound strange, but I was afraid. I was afraid that they will label me a troublemaker. So I kept silent. I was silent anyhow, but at least I didn’t say anything in writing. As the mistakes accumulated, I realized that “If I don’t speak out, I will not get out of this place as healthy as I could”, and I started to speak out. My luck was that my daughter was my voice for a while, until she had to leave. She was my patient advocate.
But many patients are threatened by us even if we are nonthreatening. But we can try to disarm them and create an atmosphere of less threat and can encourage them to talk instead of being defensive. We would say okay, let me look into it and let me do something to about it.
One of the most humiliating episodes that happened to me occurred when I was recovering from my laryngectomy. That one morning the residents were making rounds. I had a laryngectomy tube—which was completely clogged with mucus. The nurse usually came and cleaned it, but she hadn’t yet. The residents got there first. So I asked a resident to clean it. I was shocked when he took it out without gloves, went to the faucet and flushed it with water. I refused to let him put it back in my trachea – in my tracheostomy. I wrote to him, “This is not the way you should clean it. You need to open a kit and do it.”
He said to me, “We are running the show now. This is how we do it.”
I was so helpless I couldn’t do anything except refuse him from doing it. When I mentioned it to the attending (physician) when he came, he told me “Oh, this is resident is very nice. He would never behave like this. I can’t believe he did it.”
I didn’t hear anything more about it. So there was an example of the mistake. You don’t clean it with tap water! You have a kit. You need to wear gloves. This is also an example of arrogance. There is no room for arrogance.
Now if I was in a position to do it, if I could walk, I would go to the hospital director and complain but I was a sick, helpless patient. Here is an example of how a patient can’t do anything. He is completely at the mercy of staff and mistakes that are being made. So I think there is a need to better education, for greater humility, and less intimidation.
Also there are places where the nurses are not as well trained. I noticed a difference in the quality of nursing. When I was hospitalized at the Naval Medical Center in Bethesda I noticed that the nurses were young but very well-trained. Everything was done according to the book. However, when I was hospitalized at Walter Reed Army Hospital, I found out that about two thirds of the nurses were civilians, from many places. Some were good, but some were not. Some nurses were well-trained and some were not. You need to make sure that everybody is following the same procedure and that is best way to prevent mistakes.
Audience: “I think you need to go around the whole country to teach us about this. This is the tip of the iceberg. You are a physician, you are an insider, you know what happens there so you can say I have a job I don’t do much. The problem is the education that you mention. To be critical, you have to suffer pain. People like to be praised all the time, “You are doing a good job, you are doing a good job.” If one harms you, say at this time that it is wrong, so the next time you praise will be appreciated. You’re coming from a high school, a college, medical school and something and so, and told. “Be nice, not to be critical” We are not critical enough. The problem is big!”
Dr. Brook: “I couldn’t agree with you more. It’s important. At one point I said enough, I guess I’m not going to be a nice guy anymore. I am going to take the gloves off. I am extremely grateful to everybody and I say it to them. But on the other hand, I realized that we are all human beings. We all make mistakes. It’s not a perfect world and the only way we can prevent it, reduce it, is to have check lists. We need a system that reduces it. One thing is to have lesser burden on the physician, lesser burden on the nurses, so that they are not overwhelmed, so that they don’t make mistakes because they are tired and overworked.
We should have a system where people are encouraged to admit and discuss mistakes openly so we don’t repeat it. We have in our own hospital such a venue where we meet once a month and we talk about the mistakes we made–without accusing anybody, without reprimands, just to talk, to prevent the errors from happening again.”
Audience: “We have to listen to what you are saying…The part I found most important for young doctors, that we have to emphasize over and over again is the importance of a good history and a good physical exam. Some of our younger doctors think that a physical exam is complementary to the technology and it should be the other way. Technology should be complementary to the physical exam. We are missing a lot and need to go back and listen again sometimes you have to remind yourself that just because we have CT scans and PET scans, it’s not the same as talking and having the doctor patient relationship .
Dr. Brook: “I agree that we forgot the art of medicine over the years. I remember when I went to medical school in the 60s, how my teachers were really true clinicians. They could examine the patient and listen to them and talk to them and they were able to find things. Today people forgot the art of medicine. I believe that even today 95% of the diagnosis can be made by doing a good physical examination. Unfortunately the new technology made us rely on tests and scans and in this way we spend less time with the patient and that course also leads to mistakes.”
Audience: “The question I have for you is with cost being such an issue now, I think, what are we to do with less staff when there’s still a need for extra eyes?”
Brook: “I think there is no substitute for more staff. When someone is out of surgery in the ICU and in critical condition, you need a person there. I don’t think there is a substitute for that. I wrote about those episodes in my book. There was an episode when I was mistreated because of lack of personal. I had a skin flap removed from my hand to create my new esophagus. That flap needed to be constantly covered. The nurse was in the process of changing the cover when she had to suddenly leave my room because she had something else to do. I was lying there for about 20 minutes. I couldn’t call anybody. When I finally got somebody, they told me, “The nurse is on the phone ordering something.” A resident physician who came to complete the change was called away by the attending. Nobody seemed to care that I had tremendous pain for another 25 minutes. There is simply sometimes pure negligence that happens. The only thing I can tell you is that a patient advocate is so much needed. I know that if, God forbid, anybody of my family will be in the hospital, I will not leave their side 24 hours a day. Fortunately, it didn’t happen to me yet but if it will, I will not leave their side.”
Audience: “What I think this episode reveals is simply what Dr. Mary says, that there is a loss of professionalism amongst everybody involved in healthcare. There the physicians, I think have forgotten that they’re in charge of everything. We do need to hold everyone accountable. The nurses have forgotten what their true training has been in. Everybody has focused on getting the work done as quickly as possible so they can get onto the next thing. It has left the medical profession in the dark.”
Dr. Brook: “I agree with you. People are so overwhelmed. Sometimes when I wanted to talk to a physician (by writing because I couldn’t speak) he would dismiss me, “I’m really very busy now, I have to run to my clinic or I have to run to the OR. If you like, have your wife call me.”
I had one mistake that happened because the doctors wrote an order for another patient in my chart–to start feeding me one week after the surgery. It seemed to me very strange, because I remembered that my surgeon told me that I will be starting feeding two weeks after the surgery. I protested, but then I thought, “Maybe it is all right. I’m happy to eat again”. Only because I questioned it again and again, did they finally stop it–twelve hours later when they realized they made a mistake. I was fortunate that no bad thing happened because of it even though after getting the type of surgery I had, it was dangerous to be eating too soon. Here is an example of an error and I don’t even know if there were any repercussions because of it!
I wanted to let you know that you that you could read my book, “My Voice: A Physician’s Personal Experience with Throat Cancer”. It’s available for free on the Internet at my blog and also you can get it from the American Academy of Otolaryngology website ebooks site at http://www.entnet.org/mktplace/ebooks.cfm
My RCC was misdiagnosed for more than a year by a PA who felt the area on a regular basis, allowing my kidney tumor to grow and metastasize. The abdominal pains and blood in my urine were misdiagnosed and treated as a bladder infection. It was only after I demanded it was I sent to have scans done.
Sean
I agree with you Sean,
However this doesn’t apply to “ALL DOCTORS”. I’ve seen some awesome Doctor’s. Don’t get me wrong.
Today, YOU THE PAITENT ARE “your best advocate.” All to many times have I seen this same scenario happen in any cases of cancer that could have been caught much sooner had the Patient spoke up and pursued their concerns. DO YOUR OWN HOMEWORK AS WELL.
Remember, Our insurance companies put many restrictions on what your doctor can and cannot do. Worse yet, They make them follow a pretty strict protocol of what test can be performed and when! Sad but its the truth!
My approach? If my insurance Co. requires a pre authorization from my Primary, I go see him. I explain what is going on. If my primary doctor “does not specialize” in the area of concerned, (ie. Bladder infection) I ask for a referral to see a urologist! People are to afraid to speak up for themselves. If your Dr. isn’t willing to refer you!! Me ??? I’d be without doubt considering a new Primary Doctor! ( you have to use your own gut feeling)
Isn’t that why Doctors specialize in certain fields of medicine!
Medical school and internship’s cover’s a teeny tiny bit of EVERYTHING. Understandably so. There is so much to learn. A very open, transparent Dr. will tell you that is pretty much true, it takes years and years of hands on experience. No really good doctor will be offended by you asking lots of questions and or asking for a referral. Just ask your doctor if he or she specializes in your area of concern. Lets just use a bladder kidney problem for example. I can’t imagine being ill or feeling that something is really off in my body for any length of time.
REMEMBER YOU KNOW YOUR BODY BETTER THEN ANYONE. ( You live in that skin!)
Under NO circumstances, if I continue to have the same medical issues (or new symptom’s arising) and the Doc is not actively exploring other reasons that could be the cause of my issues, No offense Doctor. I’m finding a new Doctor who will be proactive….. I’ve personally lost several people who have died because they were to afraid to ask as questions! Ask, ask, ask away! There is nothing wrong with doing so! Unfortunately if you don’t, your the only one who snuffer’s the consequence’s :I(
Big Hugs to all the people going through these tough times… Remember, your mind is the strongest weapon you have against Cancer! It’s a fight that I believe can be won in many worse case scenario’s. God Bless!