Kidney cancer is generally a very silent disease. It is sneaky, hides out for years, and is often assumed to be something else. In my case, my doctor essentially decided I was just a menopausal women with the ever-popular “stress” as a an extra. The stress of carrying about a 10 cm tumor and wasting away was probably part of it.
That slow diagnosis, often delayed for years is far too typical. Only the greater use of CT scans has been significant in finding kidney cancer at an early stage. And just what is early or small? Looking for a cracked rib, or the dislocated shoulder has often revealed kidney cancer, and in the case of the shoulder, lung mets. And then the hunt is on! By the time this diagnosis is made, nearly 30-40% of kidney cancer is already metastatic.
The ‘classic triad’ of symptoms, are 1) blood in the urine, 2) flank pain, and 3) palpable mass in the abdomen. There are doctors who will consider kidney cancer only when the patient has these three symptoms, but that happens in fewer than 10% of patients. The cancer has to be pretty far along to be found this way. Meeting a pair of new doctors who were aware of my kidney cancer, they were obviously bewildered to hear that I had had none of the these symptoms. “But those are the usual symptoms,” one said. Maybe ‘classical’, but not ‘usual’. Unfortunately that expectation is a barrier to good diagnosis.
Beyond the diagnosis and the staging of the disease is the pretty obvious question of what to do next. (Staging: another of those words used one way in English, and quite another in medicine No wonder we are confused.) Getting treatment is derived from that ‘staging’. To be told your cancer is at Stage I seems the only bright spot of a cancer diagnosis, but not so reassuring with kidney cancer. The “SMALL” Stage I kidney tumor is one which is confined to the kidney (good news) and is 7 centimeters or less. Maybe Europeans react with the required, “Yipes!”, but few Americans would until they know that this is almost 3 inches in size!
Ain’t so small in my world, or in my kidney!, or anywhere else. In my previously-naive patient world, I thought a ‘small’ tumor was the size of a pea, or maybe a peanut. In any case, these so-called small tumor are Stage I, of four Stages. Don’t even ask about Stage V. Calling a near-three inch tumor small reflects the history of many very large tumors being found in the early days. Even in 1997 there was discussion about whether a 5cm (2 inch) tumor should be the ‘small’, and in the 1987 system, it had to be 2.5cm to be small, ie, about one inch a T1 stage. I do not understand why this basic staging was so dramatically changed, but it may well be that there were so few truly small tumors found in this early CT era.
In any case, we now have a system which lumps all tumors 7 cm or smaller into TI category, re-divided into T1a if under 4cm, and T1b, up to 7cms. This minimizes the sense of risk that comes with these larger Stage I tumors, despite clear evidence of much greater risk at about as they grow. That shift to a more aggressive tumor, capable of having metastatic potential, seems to start just over 1 inch, about 2.8cm. There is a measurable increase in risk of about 62% at this size, so waiting around for a mass to be palpable (ie, it can be felt) puts us all at risk. And of course, that metastatic potential has likely started even earlier, prepping the body to accept new cancer in new locations.
Thus, the absolute need to monitor patients who have had large ‘small’ tumors far more carefully and for a longer time. The reality is that even truly small tumors have the ability to start the metastatic process. Tiny and invisible even to a CT, they can grow unnoticed for several years. There is no magic ‘five years/safe at home’ for kidney cancer patients, sad to say.
So, if your doctor tells you not to worry, that he got it all, that it was small, that there is no need for further monitoring, you might just find another doctor who keeps up with the kidney cancer literature. If you got this far with this post, you may be ahead of your doctor.
Re the above risk stats, seehttp://www.cancertherapyadvisor.com/renal-cell-carcinoma/renal-cell-carcinoma-larger-tumors-high-grade-pathology/article/415189/
Being diagnosed with kidney cancer is a stunner. Facing surgery and endless, oft unanswered questions changes your life. Patients with small tumors, easily removed, are often told not to worry about it coming back. Of course, there is ALWAYS the possibility that even small “I got it all tumors” can recur. Sadly, the current guidelines fail to catch about 30% of recurrences, using the 2013, 2014 guidelines. These guidelines were from an earlier era, where there were fewer small tumors found, so there was data lacking on long-term follow-up.
We patients ask? “Why not just take the meds that the patients with metastatic disease do? Wouldn’t that prevent it from coming back? If it works to fight the mets, why wouldn’t it prevent new ones from getting a foothold? “
Why not use the meds that they use now against metastatic disease? Why wouldn’t that work? Have they tested that idea?
In February of 2015, a study was released which comparing patient response to 1) sunitinib (Sutent),2) sorafenib (Nexavar), or 3) placebo (no real medicine). This three-arm study included 1,943 patients who had locally advanced clear cell and non-clear cell histology RCCs. They were thought to be at high-risk for recurrence of their cancer, and might benefit from “adjuvant” therapy. The researchers hoped that they would see a 25% improvement in time to recurrence of disease with the meds vs no meds.. That would means that the typical 5.8 years median Disease Free Survival (DFS) would go to 7.7 years.
Sadly, there was no benefit to taking the active drugs compared to the placebo. More sad is that the patients had side effects associated with the drug, referred to as “adverse events”. In fact, many dropped out of the active agent arms into the placebo arm, certainly knowing that the med they were taking were anti-cancer meds. Those “adverse events”, severe fatigue, hypertension or hand-foot reactions, were observed in those taking the active agents and rarely in the placebo patients.
The median time on the drugs was 8 months. That means half the patients were on drugs more than 8 months and half were on the drugs less than 8 months. Even those patients starting with lower doses of the drugs fared worse than the placebo group.
Despite taking the medications and enduring the side effects, the recurrence was about the same. With medication or without, these patients, as groups, did the same. Those taking the meds had Disease Free Survival of 5.6 or 5.7 years, similar to those not taking any real meds. There was no real added benefit to these patients. Certainly the quality of the life was affected by the side effects, and the constant reminder of the spectre of more cancer.
What can patients learn from this study?
The fear of recurrence is real. After all, the expected time until the disease progressed (love using that term for cancer!), was about 5 1/2 years. These patients were carefully monitored with CTs on a regular basis, which caught their recurrences as soon as possible. Had they not been in this trial, it is reasonable to expect that many would not have received those scans and not know of the recurrence as it happened.
The reality is that the typical patient may or may not continue to be monitored. Even those who passed the 5 1/2 year mark without recurrence may not realize that RCC can come back. Again, 30% of recurrences in small, non-metastatic disease are not caught. One can assume that the higher risk group in this trial would also be at risk for that level of recurrence.
Take-home message: At present, nothing has been shown to prevent recurrence of this locally advanced disease. Even the non-metastatic small tumors that have sent out invisible “wanna-be mets”, and no one can yet guess who is at the most risk.
The best approach is to monitor yourself and your general health and to demand CT scans, especially in the lungs, where metastatic RCC is most likely to start. That does NOT mean an x-ray, as those mets would have to be about 1/4″ in order to be seen. My own lung mets were under that size when first found, but there were hundreds of them, and they grew quickly. Not visible on an x-ray, but growing every day.
Despite the disappointing study above, the ASSURE study, more clinical trials are recruiting patients for similar studies using drugs that have already been shown to be less active than those in the ASSURE study. I would be cautious in getting into such a trial, and would spend my energies seeing that my monitoring is extended at least until 10 years past my surgery–even with those “got it all” primary tumors.
Though I was lucky to receive good care, after eight precious months working with a specialist trying to figure out why I went from healthy to damned ill, it was more than good medical care that saved my life. Being diagnosed with a terminal illness is terrifying and isolating. I felt alone in a wash of pink ribbons, without anyone who understood my disease process and how to deal with it. Who gets kidney cancer?!
By some internet miracle, and at the depth of my horror at the prognosis I faced, I found ACOR–Association of Cancer Online Resources–now called www.SmartPatients.com. http://www.smartpatients.com/kidney-cancer These were other patients who provided both TLC and education that I so desperately needed. Moderated by intelligent and experienced patients and caregivers who knew what had happened to me. What I did not get was someone telling me that I had gotten sick for failure to buy their supplement or for leading a dissolute life!
I wrote a simple distress call online, that I just had a nephrectomy and was being advised to consider HD IL2 for my countless lung mets. I needed help. Within forty minutes, another patient offered his quick story with the disease, that he was working, in a clinical trial and doing better. He gave me his number and said it was a good time to call. I did call, and found a real person on the other end, who immediately let me know that I was not alone, that other options were emerging from the research, that my doctor was considered to be excellent and so on. Not only this call, a clear signal that I was not alone, but he gave me his cell number, his work number and his pager. “Call me anytime you need to talk.” With that, my head cleared every so slightly, and I began my journey to this world, one which has lasted nearly ten years. And it has led to you.
Through www.SmartPatients.com I have come to offer my own knowledge to others, and hope you will find this a valuable resource as well. You will be welcome, and given tools to make you more capable of dealing with kidney cancer. Other cancers have similar groups, of course, as we all need to be SmartPatients.
My first foray into the world of “patient” began the day I was diagnosed with kidney cancer. All my other visits with the doctor, my hospitalizations to have children, and even the odd time I received IVs of blood never had turned me into a patient. To be deemed a patient was for other people, for those who were sick, or chronically ill.
That was never me until a wish for cosmetic eye surgery led me to get a blood test and the report of extremely low red blood cell count, a hemoglobin measure. Mostly aggravated that low reading would hinder my plans to have new eyelids, I assumed my approaching menopause had shifted things a bit for me. Get “re-calibrated” with some blood, be a bit smarter about eating other than M&Ms for lunch, and all would be well.
Well didn’t happen that way. Being told by my GP to go to the ER to be admitted to test for my low red blood cell count was more an annoyance, and bewildering. The GP told me to be careful driving, as I could “bleed out”, were I in an accident. Had I taken him seriously, I might have been better off, but who wants to become a patient?
Three pints of blood, a colonoscopy, an endoscopy and a doctor assigned to me by the hospital later, I was sent home with a packet of iron pills, and reminder to eat very well, especially protein. More liver pate and red meat, and fewer M&Ms, and an improved diet would fix it all, I was told.
Months and more tests later, looking less and less healthy, losing weight, being polite to the doctor, being on time and starting to fade away, I did not know that I was dying. As I could later determine from the doctor’s notes, he thought I was an alcoholic in need of a liver biopsy to “confirm the cirrhosis”. That biopsy required an ultrasound, and the race was on.
The ultrasound tech was chatty and friendly, until a sweep of her wand across my lower right belly. She turned herself and her screen away from me and stopped talking. Knowing the liver was on the left, and her wand was on the right, I had a pretty good idea that the kidney was the new problem area. Of course, my questions went unanswered, but was told that I would have a CT scan later than day. But still no answers.
Still in the flimsy hospital gown, I discussed with my husband what was likely my new kidney cancer diagnosis, and figured I would just get a neat little incision, where they could take out the neat little tumor and I would get on with my neat little life. Off to the CT scan, with more techs discussing me, carefully out of earshot, ignoring my pleas to explain what had been found. “You doctor will talk to you” was the non-response.
But he was pretty non-responsive as well, waiting until late in the evening before telling me what I already knew, that I had a mass on my kidney. Masses don’t belong there, so it must be cancer, but he was unwilling to affirm that. He would find me a urologist the following day, he promised.
That recommendation given without further info, and in light of the frantic internet search, I was not enthusiastic about his recommendations, and especially when the urologist failed to mention any expertise with kidney cancer on his website. Ain’t a good sign, says I, so plan B was to get to the Mayo Clinic.
I had grown up in western North Dakota and had learned that fancy health problems spurred a trip to Rochester, Minnesota. Within a few days, I was in the Mayo Clinic, going through a series of new tests and imaging with the urologist appointment at the end of the day. Try to coordinate that in less than 24 hours, and you will appreciate the miracle of Mayo.
At that appointment, my neat little tumor was now described as a malignant mass, about the size of a softball. It had pushed the kidney up toward the liver, and thus caught the attention of the US technician. Bad enough, I thought, but the subsequent CT had also shown my lower lungs to be full of tiny mets. Mayo’s more thorough CT showed my entire lungs to be filled with tiny white metastases. Not only did I have a huge tumor, my lungs were essentially a tumor colony.
Stunned, and nearly deafened by this news, I struggled to hear the doctor say, “I have a plan for you.” With that hope and that plan, I began to breathe again. And have been doing so for the last 10 1/2 years.
Thanks to so many people at Mayo, including Dr. Brad Leibowich, his staff, the angel nurses, and the Mayo brothers who created this wonderful place.
The lovely cliche, “We are all patients” is just that. At every medical conference, or in the new lobby of the hospital, that phrase is offered. While it is true in a statistical sense, it has a snarky sound to the new patient, reeling from his induction into the medical world, foreign and threatening. It can really seem snarky to those who know how poorly patients can be treated, how overwhelming the language of illness is, and how chaotic a hospital setting is for most.
The patient experience for someone who speaks the language, whose friend is a specialist, or can understands the imaging reports and lab values, is in stark contrast for those lacking such resources. Not much we-ness in those two patient groups!
Certainly the medical people who suddenly become patients, or are thrust into being a caregiver, can offer their own colleagues insight into those new roles. But rarely is the newly diagnosed patient, one who has never “known” how the system works ready to take on this role. He is often the patient at the greatest risk–especially when told, “Be your own best advocate.” Most of the time, that “Be your best” does not give the patient anything, but a reminder of how lost he is.
The recent convert to patienthood who can navigate the system may be a wonderful translator of the dialect and the cultural mores of that system, but with limited impact. If that medical pro turned patient is not also willing to change that culture, to be more open, to provide ready access to information, and to teach to the wider world, most patients will not be well-served by this new awareness. As a society, we will continue to be inefficient in our care of the sick, have poorer individual and community health, and waste incredible sums of money.
Patients could be given readable information about what the standard of treatment is for their disease. They can learn that the oncoloigst should recommend more frequent imaging, or that there are other treatments than the scalpel and chemotherapy. They can learn how to enhance their daily health, how to monitor side effects, to clarify their own health concerns. Patients can be guided to credible online resources or patient groups so they can ask the new question, compare notes, learn the changing vocabulary.
Doctors can tell patients that diagnosis is tricky and requires testing and feedback along the way. They can remind patients of the uncertainty and complexity of cancer, or a chronic disease. They can welcome questions about side effects, new studies, and treatment options. The dynamic will shift as the patient becomes more knowledgeable, or has greater medical needs, and the doctor must shift as well.
Patients and their providers need to partner with one another, with the patient at the center of all those relationships. The patient needs ready access to his records, information relevant to his needs, and an atmosphere of collaboration, appropriate to the moment. Anything less is damaging and wasteful, and we ain’t got time and money for business as usual.
We hear about gene sequencing and personalized medicine, and yet few of us really understand what that means. All of this, despite the hype! We also hear about targeted therapy. As a minimum that should mean that doctors are targeting the tumor for destruction, but is not that easy. As usual.
The University of North Carolina researchers have done critical reviews of clear cell kidney cancer. They questioned why there is such wide variation in the aggressiveness of clear cell RCC (ccRCC). Almost all ccRCC looks alike under the microscope, the usual “pathology” report, but tumors don’t behave the same. Some are shockingly aggressive in their growth, even the small ones. They metastasize quickly, and break the surgeon’s “got it all” prediction. The overall survival (OS–the longer, the better!) is wildly different, despite the similarity.
If this is the same kind of cancer, why does it behave so differently?
The obvious answer is that these tumors are not really the same biologically. That can be shown by an inside look at the tumor’s DNA and patient’s normal kidney DNA. This is what gene sequencing can do, i.e., help define what differences exist in the tumor cell. This is essential in “targeting” the treatment to the tumor. You have to see the recognize what IS the target to hit it with the right treatment.
This linked YouTube lecture below helps explain these new terms. It gives me appreciation for the challenge faced by researchers, clinicians and patients in getting proper treatment. And nobody cares as much as we patients!
Dr. Kimryn Rathmell and colleagues at U of NC created a test which can differentiate the more aggressive form of clear cell kidney cancer from a less aggressive form. Should one monitor a smallish tumor, monitor a patient more closely after surgery, or just assume everything is fine and dandy? These tests help in that decision. (PS Don’t forget that a “small” Stage 1 kidney cancer tumor can be the size of a golf ball. “Regular” size Stage 1 tumor can be the size of a nice tomato. Small, indeed.)
We’ve learned it isn’t just “cancer”. It’s not just “kidney cancer”. It’s not even just just “clear cell” or “papillary” or “chromophobe”! Instead it is a molecularly defined cancer which has taken up residence in one’s kidney. Different drivers, some more aggressive than others–big surprise. Different strokes for different folks, and different targets for different testy genes in our tumors!
https://www.youtube.com/watch?v=Y9HumO20GKc A transcription can be found in “Genetic Sequencing for Dummies and Me”
Most people are not surprised that there is no ONE thing called cancer. Tumors in all the organs or invasive cells in the blood or bones are referred to as cancer, but start when cells go wrong, whatever the cause. As soon as you are told you cancer, whatever it, the quest begins to find out exactly which cancer it is. With kidney cancer, or its more melodious name, renal cell carcinoma, there seem to be endless variations on what may be called kidney or renal cancer. To treat it requires a very careful analysis of what is really is, starting with the pathology of the tumor when it is biopsied. With kidney cancer that biopsy is usually done after surgery for the tumor. That biopsy will describe the shapes and type of cell in the tumor, which can be mix of types. And then the real work begins.
A recent article in “European Urology” reviewed the mix of HEREDITARY renal cancers, those that arise due to one’s background. More common are the “sporadic” kidney cancer that could arise out of the blue or in response to some environmental toxin. There are ten Heredity Renal Cancers, or HRCs. My goal is to alert the reader to the possibility that his cancer might be one of these. This would affect treatment, and may suggest the need to test family members.
If you have kidney cancer or RCC, you may be familiar with “clear cell” or “papillary” to refine the description of the cells in the tumors. This may not be the whole story, as those HRCs—the hereditary kinds—may manifest a mix of ways, including as clear cell or papillary histology.
The most common HRC is Von Hippel-Lindau (VHL) disease, with both benign or malignant tumors. RCC can be found in a 24-34% of VHL patients, appearing at mean age 39 years (far younger than non-heredity RCC), and often with multiple tumors and in both kidneys. Cysts which appear not to be malignant must be watched–they have the potential to become malignant over time. Generally they are managed based on the size of the largest of these lesions. Clear cell RCC is the one VHL-related subtype.
Hereditary papillary renal carcinoma (HPRC) is rarer, and typically occurs later in life. Papillary tumors are the only phenotype with HPRC, and patients often develop numerous tiny tumors, 1000 or more. These tumors are considered type 1 papillary renal cell carcinoma (pRCC) with a low nuclear grade, monitored with CT scans, and some do metastasize, though this is rare. The MET gene is implicated in the growth of these tumors.
Hereditary leiomyomatosis and renal cell cancer (HLRCC) is newly identified as a HRC. Rarely do patients develop RCC, but are susceptible to developing multiple leiomylomas, which are generally benign. When there is early onset of HLRCC, then RCC is found in about 20% of those patients. These tumors can be aggressive, and about 2/3 display a papillary pattern. Such tumors tend to be hyper-vascular.
Birt-Hogg-Dube (BHD) syndrome is quite rare, about 1 in 200,000 people, and thereby likely under diagnosed. This raises the risk of developing kidney tumors, which occurs in 25-35% of BHD patients, and at mean age of 50. These tumors have varying histologic subtypes, generally chromophobe RCC or hybrid variants. And there can be variants in the same tumor or within the kidney. There is a risk of metastases, though rare. The characteristic skin lesions of BHD syndrome are not malignant.
Even more rare is Tuberous Sclerosis Complex (TSC), which can manifest itself in renal lesions, cysts and occasionally, RCC, the latter at a young, average age 28. Neurologic complications can accompany this syndrome.
SDHB-associated paraganglioma/phaeochromoytoma is another heredity condition which may give rise to a mix of renal tumor, including clear cell RCC, chromophobe RCC and oncocytomas, i.e., a mix of histologically different types.
An HRCmay be suspected in patients with a family or individual history of renal tumors, in the instance of both kidney having tumors, or one kidney having multiple tumors or in early-onset renal tumor, i.e., under 50 years of age.
Clinical diagnosis can be further refined by genetic testing, and thorough review by an experienced uropathologist is fundamental to the diagnosis. First consideration would be a VHL analysis and genetic analysis of SDHB and FLCN genes, as warranted. Patients with type 1 papillaryRCC should be considered for MET analysis. The presence of clinical symptoms related to any of the syndromes will guide the gene screening. Testing on family members may well be warranted.
With these cancers, it is possible to have multiple lesions and affect both kidneys. Thus, treatment should preserve renal function and control the risk for metastases. Use of ablation to retain maximum renal function may be preferable to partial nephrectomies, for example.
Though these heredity renal cancers arise in a different manner than the more common sporadic RCC, the study of the molecular pathways provide some insight into new therapies for those patients as well. Thanks always to those researchers who help in this struggle for information, as that is essential to provide treatments.
Delays in being diagnosed with my kidney cancer may have led to it going to my lungs. Bad enough, but I had good care in my treatment–I think. Rarely can a patient analyze his own care for errors. No so with this guest writer, Dr. Itzhak Brook, whose story of his misdiagnosis and numerous treatment errors is one we should read. With rare insight and passion, Dr. Brook is dedicated to prevent medical errors. The following is from his lecture at LSU Health conference in May 8, 2013.
Preventing Medical Errors:
A Physician’s Personal Experience as a Laryngeal Cancer Patient
Dr. Itzhak Brook: Guest Speaker at LSU Health conference in May 8, 2013.
Dr. Brook is introduced: Dr. Brook has written 700 articles. He is an associate editor of several medical journals. He is a member of the editorial board of several medical journals.
I have been very fortunate to serve with him in the “Head and Neck Cancer Alliance National Committee.” That’s where I got to know Dr. Brook, and he is doing some amazing work in terms of lobbying for head and neck patients to get their voice prostheses, electrolarynx, basic functional components that are not covered by healthcare.
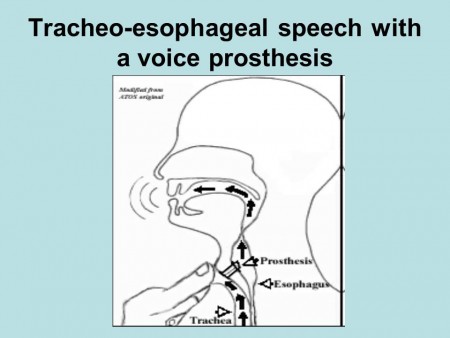
Dr. Brook was diagnosed with larynx cancer in 2006. Two years later he had to have a laryngectomy, and he currently speaks with the tracheal esophageal puncture. He is the author of the book, “My Voice: A Physician’s Personal Experience with Throat Cancer.” In fact, this morning he gave our department an inspiring talk on how it is to be a laryngectomy patient, and what we as physicians should look for. Dr. Brooke is the recipient of the 2012 John Connelly Medical Ethics Award by our Academy this year. Once again I would like to welcome him.
Dr. Brook speaks: “Thank you. It’s a pleasure to be here today and to talk to you about medical errors. First of all, I hope that you can all hear me. I have a very low voice when I speak. I speak with the voice prosthesis. Here is a diagram of how I speak. I do this by diverting air through a little prosthesis into the esophagus and where the air and the vibrations created allow me to speak. This is my challenge: to be able to maintain the seal with this device around my neck which allows me to speak. I wanted to talk to you today about my experiences as a patient with throat cancer and how I encountered many of these errors from nursing, then physicians while I was patient, and how I suggest we can prevent those errors by better education, patient advocacy, and how we can improve patients’ care.
It was shocking to me –when I became a patient to realize how common they are. I have been a physician for more than 40 years, but I had never been on the other side of the stethoscope. As a physician learning on my own the seriousness of those errors, there wasn’t a day in which I did not notice two or three errors that were done by nurses, physicians, technicians, nutritionists.
It was psychological and physical strain to be on the watch all the time to try to prevent errors. I realized that hospitals are very dangerous places to be. Not that I didn’t know it, but this really illustrated how it’s a miracle that patients get out without more damage than they came in with. Indeed in surgery, it’s estimated that about a third of all patients end up with some kind of permanent or temporary damage because of mistakes.
Imagine how lucky that I was the medical professional, that I was able to observe those errors. The layperson is much more susceptible to them and cannot even correct them. Many patients are intimidated and are so grateful to us that they don’t voice their concerns or criticisms. That is why we don’t hear, and we don’t prevent many errors that can be prevented–even when they are observed. People like myself who have difficulties in speaking, especially after surgery when I could not speak for six weeks, are much more susceptible to such errors.
Let me share with you, first of all, what I saw in my own eyes as far as the errors I encountered. The first one that I noticed was that my physicians failed to recognize that my cancer had returned–even though I came to them with complaints of pain. They relied on an imperfect physical and endoscopic examination. They relied on the fact that the CT, MRI and PET scans were all negative.
But there was no substitution for a good physical exam which they neglected to do. What they should have done was asked me to do a Valsalva maneuver while doing an endoscopy, to breathe air and hold it and then look. This allows parts of the upper airway, most specifically the pyriform sinus to open, which reveals an area that is otherwise not seen. My tumor was already an inch long and it was missed by CT, MRI and PET. That was an example that the diagnosis can be made in many cases by good physical exam.
The other thing that I learned is that some of the mistakes were because of the physician’s lack of experience. My surgeons offered me a procedure which they had only done once before. I was desperate to get the cancer out and neglected to think about it myself, as “You need this procedure, but there may be people across the country who have done it hundreds of times.” What they told me is, “In surgery you see one, you do one, and you teach one.” I believed it, but I know it now it should be, “You see 1000, you do 100, and then you teach one.” This is the reality of the world.
As physicians, we like to help our patients, but we should know our limitations, and in fact, that we are not able to be expert in everything. It’s okay to admit it and refer patients to people who know more. Some cancers are so rare, like larynesophageal cancer, thanks to fact that less people smoke and drink, even at the Centers of Excellence, their number is limited. It’s okay to admit that some procedures are better done by those who do them more often. The fact that they removed scar tissue from me instead of the cancer speaks to my surgeon’s inexperience in the technique they used.
Another error I noticed was that my physicians wrote my orders in the wrong chart. Consequently I did not get the right treatment and I got therapy for another patient. This occurred in one of the best medical centers in New York City. You can appreciate that even in the best places mistakes do happen, and these are just a couple of several errors my physicians’ made in my care.
Nursing errors are more common and range from not responding to calls to forgetting to connect the call button to my bed. I was in ICU a day after my laryngectomy, and my bed was only three feet away from the nursing station. I was connected to five different tubes, IV lines, catheters. Suddenly I was choking with secretions. I couldn’t cough them out so I looked for the button to call the nurse. I could not find the button that fell to the floor because it was not attached to the bed appropriately. To save money the same nurse was serving two other ICU patients. My nurse was away. I couldn’t call for help. disconnected my PO2 monitor. Nobody came. I disconnected the EKG monitors. I thought they would see a flat line.
Nobody came. Fortunately, my wife just happened to come in the morning, and she called the nurses to suction me.
Imagine that this can happen in ICU. You can choke to death! Not every hospital has one nurse for three patients. When I was first hospitalized in military hospitals they had one nurse per patient. But in that hospital in New York, they were saving money. So here’s an example of a serious nursing error.
Some of the errors are listed here–like not washing hands, not covering the thermometer with the plastic cover, using the improperly sized blood pressure cuff, leading to alarming results. That meant I got medications to lower my blood pressure which wasn’t high, and administering the wrong dose of medication. So these are some of the mistakes.
There is a lot that can be done to prevent errors when better and uniform methods are used for training.
What is important is to adhere to certain standard of care. The rule now is to use algorithms and check lists. Algorithms have been shown to prevent many errors. Simply by following the chart, you don’t forget about it; reviewing the records to detect errors and to admitting it and training the personnel to prevent it. There are people who keep making mistakes—those individuals should be retrained or even dismissed. They should be reprimanded.
It’s also important to have better supervision and encourage patient advocacy. Encourage patients to talk about those errors. Admit them if you think you made a mistake. Admit it and don’t try to wash it away. Admitting will prevent malpractice suits. Patients who see that the personnel acknowledged their errors will be less likely to seek reparation. If they don’t see it they are more likely to look for punishment.
That is why open discussion is important. Encourage patient advocacy. Tell them the truth. Tell them the treatment plans. Let them be your eyes and ears, so they can come and correct, and tell you if something went wrong. It’s important to ask friends or advocates to help patients make the right choices so that mistakes are not being made. Encourage second or even third opinions. There is nothing demeaning about it. It will also make the patient know that you are there to help them choose the right treatment.
What patients should do is look for the experts in their illness field. Sometimes patients make mistakes by confusing friendliness with expertise. I made those mistakes. My physicians were lovely human beings, but still those that I initially saw did not have the best expertise in my illness field.
Ask for the true prognosis. Don’t be always optimistic, but realistic so if things don’t work right, the patient should know, recognize and accept it. What I tell patients to ask for, and you should also encourage them to do is to give you their best history. The more you know, the easiest to it is to prevent errors. All the past history, all the little nuances that patients can tell will help their doctors make the right choices. Also what I ask the patient to do is to challenge us. Ask questions. Don’t dismiss these questions. We the physicians should not overshadow our patients. Let them ask. They may not always know something. Tell your patients, “Don’t assume that we the doctors know everything because we don’t.”
Medicine is as much an art as it is science. If the patient has an advocate, they are going to be more likely to catch errors and explain and ask questions, especially when the patient is sleepy or sick. Have a friend or family member be there and challenge us if necessary will prevent errors.
All physicians including surgeons need to listen to thire patients. We are all overworked, but we need to recognize how overwhelmed the patient is. They cannot always make good judgments. They are scared. They want to be saved and helped and they don’t always ask the right questions. You need to let them have time to question you, to challenge you. The more explanation you give, the better they will be in helping you prevent mistakes.
Don’t forget to examine the whole patient, not just the area where you specialize in. I especially ask my surgeons to examine on the entire body. I asked my surgeon to listen to my lungs, he said, “I really wouldn’t even know how to do it that. I’ll call the internist.” I was shocked o hear it, but at least he recognized it as his shortcoming.
You need to remember the patient is made up of body and mind. Don’t forget to think about the patient’s psyche as well and the all other issues that are psychological. They all contribute to what we call the whole patient. It’s important to recognize thoseissues and educate the young medical generation, the residents and fellows about those issues. Residents follow us, the attending. If they see us, the attending, to be patient and concerned they’ll do the same. That’s why it’s important to follow those guidelines
It is important to educate the young generation to make sure they develop good treating habits and will care for the patient and will catch errors and be more humane and caring.
I summarized a lot of what I talked about today on my blog which is listed here (http://dribrook.blogspot.com/) where I discuss also medical errors. I have a page on my blog that discusses how to prevent medical errors and what were my own experiences. This is a difficult, and a challenging topic. We can prevent many of those errors by encouraging better adherence to standards of care, patience, vigilance and advocacy. By preventing making mistakes we will get better results and better patients satisfaction.
I want to thank you for your attention. I will be happy to answer your questions. Thank you.”
Questions from the audience:
Audience; “One of my observations and thank you for presenting. My observation is that one of the major problems with medical errors is that most people don’t care or they think it is someone else’s responsibility. We don’t recognize our responsibility. Something else to the younger generation: they need to they need to feel confident enough that they will allow patients or advocates to challenge us. There are many physicians who are either overly self-righteous or afraid that when they’re challenged, their entire being has been challenged. They don’t feel comfortable enough to have a discussion like that with the patient or advocate.”
Brooks: “You are correct. Many physicians are threatened. Many come in today with the Internet more knowledgeable. Many patients know a lot about their illnesses and the more I think: the more they know, it is better. On the other hand, there is lot of false information that the patients have through many sources of knowledge that are not perfect. I think that we should encourage it. I don’t think we should see that as a threat to us. Get patients, let patients challenge us.
I can tell you that as patient I was afraid to challenge my doctors. I was so grateful initially that they were taking care of me, that I was afraid that if I would challenge them, they wouldn’t give me the best treatment. It may sound strange, but I was afraid. I was afraid that they will label me a troublemaker. So I kept silent. I was silent anyhow, but at least I didn’t say anything in writing. As the mistakes accumulated, I realized that “If I don’t speak out, I will not get out of this place as healthy as I could”, and I started to speak out. My luck was that my daughter was my voice for a while, until she had to leave. She was my patient advocate.
But many patients are threatened by us even if we are nonthreatening. But we can try to disarm them and create an atmosphere of less threat and can encourage them to talk instead of being defensive. We would say okay, let me look into it and let me do something to about it.
One of the most humiliating episodes that happened to me occurred when I was recovering from my laryngectomy. That one morning the residents were making rounds. I had a laryngectomy tube—which was completely clogged with mucus. The nurse usually came and cleaned it, but she hadn’t yet. The residents got there first. So I asked a resident to clean it. I was shocked when he took it out without gloves, went to the faucet and flushed it with water. I refused to let him put it back in my trachea – in my tracheostomy. I wrote to him, “This is not the way you should clean it. You need to open a kit and do it.”
He said to me, “We are running the show now. This is how we do it.”
I was so helpless I couldn’t do anything except refuse him from doing it. When I mentioned it to the attending (physician) when he came, he told me “Oh, this is resident is very nice. He would never behave like this. I can’t believe he did it.”
I didn’t hear anything more about it. So there was an example of the mistake. You don’t clean it with tap water! You have a kit. You need to wear gloves. This is also an example of arrogance. There is no room for arrogance.
Now if I was in a position to do it, if I could walk, I would go to the hospital director and complain but I was a sick, helpless patient. Here is an example of how a patient can’t do anything. He is completely at the mercy of staff and mistakes that are being made. So I think there is a need to better education, for greater humility, and less intimidation.
Also there are places where the nurses are not as well trained. I noticed a difference in the quality of nursing. When I was hospitalized at the Naval Medical Center in Bethesda I noticed that the nurses were young but very well-trained. Everything was done according to the book. However, when I was hospitalized at Walter Reed Army Hospital, I found out that about two thirds of the nurses were civilians, from many places. Some were good, but some were not. Some nurses were well-trained and some were not. You need to make sure that everybody is following the same procedure and that is best way to prevent mistakes.
Audience: “I think you need to go around the whole country to teach us about this. This is the tip of the iceberg. You are a physician, you are an insider, you know what happens there so you can say I have a job I don’t do much. The problem is the education that you mention. To be critical, you have to suffer pain. People like to be praised all the time, “You are doing a good job, you are doing a good job.” If one harms you, say at this time that it is wrong, so the next time you praise will be appreciated. You’re coming from a high school, a college, medical school and something and so, and told. “Be nice, not to be critical” We are not critical enough. The problem is big!”
Dr. Brook: “I couldn’t agree with you more. It’s important. At one point I said enough, I guess I’m not going to be a nice guy anymore. I am going to take the gloves off. I am extremely grateful to everybody and I say it to them. But on the other hand, I realized that we are all human beings. We all make mistakes. It’s not a perfect world and the only way we can prevent it, reduce it, is to have check lists. We need a system that reduces it. One thing is to have lesser burden on the physician, lesser burden on the nurses, so that they are not overwhelmed, so that they don’t make mistakes because they are tired and overworked.
We should have a system where people are encouraged to admit and discuss mistakes openly so we don’t repeat it. We have in our own hospital such a venue where we meet once a month and we talk about the mistakes we made–without accusing anybody, without reprimands, just to talk, to prevent the errors from happening again.”
Audience: “We have to listen to what you are saying…The part I found most important for young doctors, that we have to emphasize over and over again is the importance of a good history and a good physical exam. Some of our younger doctors think that a physical exam is complementary to the technology and it should be the other way. Technology should be complementary to the physical exam. We are missing a lot and need to go back and listen again sometimes you have to remind yourself that just because we have CT scans and PET scans, it’s not the same as talking and having the doctor patient relationship .
Dr. Brook: “I agree that we forgot the art of medicine over the years. I remember when I went to medical school in the 60s, how my teachers were really true clinicians. They could examine the patient and listen to them and talk to them and they were able to find things. Today people forgot the art of medicine. I believe that even today 95% of the diagnosis can be made by doing a good physical examination. Unfortunately the new technology made us rely on tests and scans and in this way we spend less time with the patient and that course also leads to mistakes.”
Audience: “The question I have for you is with cost being such an issue now, I think, what are we to do with less staff when there’s still a need for extra eyes?”
Brook: “I think there is no substitute for more staff. When someone is out of surgery in the ICU and in critical condition, you need a person there. I don’t think there is a substitute for that. I wrote about those episodes in my book. There was an episode when I was mistreated because of lack of personal. I had a skin flap removed from my hand to create my new esophagus. That flap needed to be constantly covered. The nurse was in the process of changing the cover when she had to suddenly leave my room because she had something else to do. I was lying there for about 20 minutes. I couldn’t call anybody. When I finally got somebody, they told me, “The nurse is on the phone ordering something.” A resident physician who came to complete the change was called away by the attending. Nobody seemed to care that I had tremendous pain for another 25 minutes. There is simply sometimes pure negligence that happens. The only thing I can tell you is that a patient advocate is so much needed. I know that if, God forbid, anybody of my family will be in the hospital, I will not leave their side 24 hours a day. Fortunately, it didn’t happen to me yet but if it will, I will not leave their side.”
Audience: “What I think this episode reveals is simply what Dr. Mary says, that there is a loss of professionalism amongst everybody involved in healthcare. There the physicians, I think have forgotten that they’re in charge of everything. We do need to hold everyone accountable. The nurses have forgotten what their true training has been in. Everybody has focused on getting the work done as quickly as possible so they can get onto the next thing. It has left the medical profession in the dark.”
Dr. Brook: “I agree with you. People are so overwhelmed. Sometimes when I wanted to talk to a physician (by writing because I couldn’t speak) he would dismiss me, “I’m really very busy now, I have to run to my clinic or I have to run to the OR. If you like, have your wife call me.”
I had one mistake that happened because the doctors wrote an order for another patient in my chart–to start feeding me one week after the surgery. It seemed to me very strange, because I remembered that my surgeon told me that I will be starting feeding two weeks after the surgery. I protested, but then I thought, “Maybe it is all right. I’m happy to eat again”. Only because I questioned it again and again, did they finally stop it–twelve hours later when they realized they made a mistake. I was fortunate that no bad thing happened because of it even though after getting the type of surgery I had, it was dangerous to be eating too soon. Here is an example of an error and I don’t even know if there were any repercussions because of it!
I wanted to let you know that you that you could read my book, “My Voice: A Physician’s Personal Experience with Throat Cancer”. It’s available for free on the Internet at my blog and also you can get it from the American Academy of Otolaryngology website ebooks site at http://www.entnet.org/mktplace/ebooks.cfm
I love this study, as it really symbolizes the tremendous change that has occurred in kidney cancer treatment these last 6 years. It is remarkable that the 124 patients are described as having already received first- line treatment, and were now in their second-line. These same metastatic patients might have received neither just six years ago.
The study was really not to compare the response to the treatments received, whether Sutent (sunitinib), Nexavar (sorafanib), or placebo. (Why any party chose or was chosen to receive a placebo is another, darker question.) That the median follow-up was 80 months is a triumph by itself. This is in contrast to the clinical trials that often show just a few months extra time which we and politicians can focus on, when the reality of much longer responses is clearly shown here. Of course, these longer survival times came from those trials which showed those few months–and this shows the reality of many more months and years of life!
Metastatic tumor burden(TB) was measured, based on the size of the sum of the longest unidimensional diameter of each targeted lesion. The additional increase of 1 cm (about 3/8”) was significant in predicting response to the medications. Siimply, adding the one-direction measure of the lesions and comparing them showed that more tumor was a bigger problem.
One can also assume that to remove as much tumor as possible may be helpful in maximizing the benefit of the meds given, although this study does not address the actual types and locations of the mets, nor indicate why no other therapies, surgery or ablation, were used. With 124 patients this would represent a mix of individual experiences, more like the typical patient group.
What does “median follow up of 80 months” really mean? A median is not an average, but a measure of the time point at which ½ of the population studied had follow up less than 80 months and ½ had follow up for more than 80 months. Since this is considered a long time in clinical trials and becomes more of a longitudinal study, we may never know the average length of time that these patients had either PFS (Progression Free Survival—time until the mets began to grow again) or OS (Overall Survival). In any case, we are aware that following this second-line of treatment, there are still more therapies and interventions which may be available. And even more options are up for FDA approval as I write.
All these options and the greater success of each muddies the study waters, but clarifies the hopes of those with metastatic RCC, or are at risk. This study proves that tumor burden (TB) is a disadvantage. Most patients have naturally assume that more cancer is worse for you than less cancer—who knew? But this gives weight to the notion that the removal of some tumors, if not all, can be beneficial used with targeted therapies. In the past, some oncologists have discouraged additional surgery in the light of metastases, with the implicit message, “It’s too late, and won’t help you anyway.” Not the doctor for me.
The story is quite different right now, but patients may need to tell this to their doctors–in the language that the doctor speaks. Certainly, there was a time at which doing more surgery for mRCC patients added little, if anything, to survival and probably even less to the quality of life. That no longer is the case, and those older studies no longer have meaning. While each patient must be treated as an individual, in light of all the variables that impact his health, there is increased optimism for the metastatic patient. Aggressive and early treatment can no doubt extend life and make it worth living.
Every family who encounters cancer has a struggle, but nothing seems harder to bear than the stories of those who are hit when they are especially vulnerable. When I was diagnosed, my youngest was barely 17, but the others were grown and independent. When cancer hit this family, they had a newborn. Against all odds, this a success story, and one which reminds us of the value of love and strength. I introduce the story of Cameron Von St James and his wife Heather, in this guest post:
“More than once, my wife has made the comment to me that she doesn’t know how I coped when she was diagnosed with cancer. Her mesothelioma diagnosis came only three months after she gave birth to our daughter Lily. What was a joyful, happy time in our lives turned quickly into a time filled with fear and uncertainty. When Heather’s doctor told her about her cancer, I looked at her, and she broke down crying. I didn’t know how we would get through this.
I was so overwhelmed with emotion. I was on the verge of breaking down when the doctor’s words brought me back to reality. He was talking about making medical decisions for my wife, and I knew this was just the beginning. It was the first of many days where we would be forced to make impossible decisions while going through overwhelming emotional turmoil.
My overwhelming emotions didn’t stop there, however. Following her diagnosis, I was angry at the world. I felt like it wasn’t fair that we had to go through this. For a while, I often lost control and lashed out at others. I used a lot using profane language. It didn’t take me long to realize how selfish I was being. The last thing my wife needed was to see just how scared I really was. I knew I needed to get it together and be strong for Heather, but it was so hard for me to do. When I was able to do it, I finally became the rock that she needed.
I was still overwhelmed with the new responsibilities that fell on me. I had a mile-long to-do list that included everything from travel arrangements to work to taking care of my house and family. I wouldn’t have been able to get through any of it without the help offered by our family and friends. I learned to prioritize and to first get done the things that were most important. I was still overwhelmed even with all the help, but I managed to get through it.
The hardest part of it all was sending Lily and Heather to South Dakota for two months following Heather’s surgery in Boston. I knew that I couldn’t work and take care of Heather while she recovered, and that’s what forced us to make this difficult decision. Heather’s parents in South Dakota offered to take care of them while Heather recovered and prepared for the next round of her mesothelioma treatment, and we decided to accept the offer. During that two-month period, I saw my family only once. I left work on a Friday night and drove 11 hours in a snowstorm to see them. I had to make the 11-hour drive home that Sunday so that I could be back at work on Monday morning.
What I learned through all of this is how lucky we were to even have difficult decisions to make. I was so lucky to have the help I had from all of our friends and family. I couldn’t have done half of what I did during this difficult time without their help. You have to accept help when it is offered to you during times this difficult. It’s been six years since Heather was diagnosed, and despite the overwhelming odds against her, she’s happy and healthy now, and cancer-free. I only hope that my words can help someone else who is going through cancer.”



The lovely cliche, “We are all patients” is just that. At every medical conference, or in the new lobby of the hospital, that phrase is offered. While it is true in a statistical sense, it has a snarky sound to the new patient, reeling from his induction into the medical world, foreign and threatening. It can really seem snarky to those who know how poorly patients can be treated, how overwhelming the language of illness is, and how chaotic a hospital setting is for most.
The patient experience for someone who speaks the language, whose friend is a specialist, or can understands the imaging reports and lab values, is in stark contrast for those lacking such resources. Not much we-ness in those two patient groups!
Certainly the medical people who suddenly become patients, or are thrust into being a caregiver, can offer their own colleagues insight into those new roles. But rarely is the newly diagnosed patient, one who has never “known” how the system works ready to take on this role. He is often the patient at the greatest risk–especially when told, “Be your own best advocate.” Most of the time, that “Be your best” does not give the patient anything, but a reminder of how lost he is.
The recent convert to patienthood who can navigate the system may be a wonderful translator of the dialect and the cultural mores of that system, but with limited impact. If that medical pro turned patient is not also willing to change that culture, to be more open, to provide ready access to information, and to teach to the wider world, most patients will not be well-served by this new awareness. As a society, we will continue to be inefficient in our care of the sick, have poorer individual and community health, and waste incredible sums of money.
Patients could be given readable information about what the standard of treatment is for their disease. They can learn that the oncoloigst should recommend more frequent imaging, or that there are other treatments than the scalpel and chemotherapy. They can learn how to enhance their daily health, how to monitor side effects, to clarify their own health concerns. Patients can be guided to credible online resources or patient groups so they can ask the new question, compare notes, learn the changing vocabulary.
Doctors can tell patients that diagnosis is tricky and requires testing and feedback along the way. They can remind patients of the uncertainty and complexity of cancer, or a chronic disease. They can welcome questions about side effects, new studies, and treatment options. The dynamic will shift as the patient becomes more knowledgeable, or has greater medical needs, and the doctor must shift as well.
Patients and their providers need to partner with one another, with the patient at the center of all those relationships. The patient needs ready access to his records, information relevant to his needs, and an atmosphere of collaboration, appropriate to the moment. Anything less is damaging and wasteful, and we ain’t got time and money for business as usual.