Looks don’t matter in kidney cancer as much as they used to, as more information comes to us about the molecular or biological nature of the diseases which fall under the “kidney cancer” umbrella. Can those important biological differences be seen in the pathology laboratory? Must we rely on next generation sequencing to determine which of the subtypes we might have?
Recent work by Dr. James Brugarolas and colleagues is reassuring. Even as they found new subtypes of clear cell renal cell carcinoma, they have also determined that these differences can be seen the pathology lab.
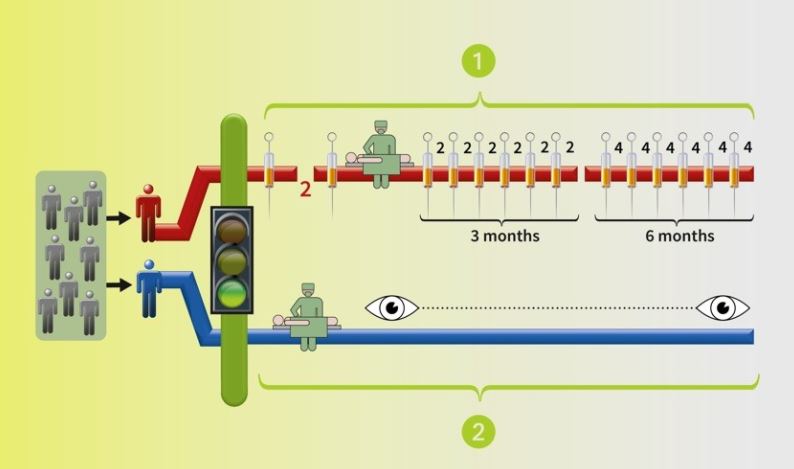
Why is this important? So-called similar tumors may behave in quite different and more aggressive ways, so this is vital to understand the threat of recurrence from a very small tumor. The affects monitoring and eventually will be helpful in drug selection.
An interview at the 13th International Kidney Cancer Symposium October 2014
https://www.youtube.com/watch?v=tCoLwClv0tw
Cut and paste the above youtube address into your browser to be able to hear the lecture, while following along below. The questions are in bold face.
Dr. James Brugarolas Discusses Biologically Classifying Kidney Cancer
“What we have learned with the development of next generation sequencing (NGS) is that no two tumors are the same. Every tumor has different mutations. Mutations are the drivers of tumor biology. With the advances of next generation sequencing, we have been able to identify and group different subtypes of kidney cancer, according to their mutation status.
Specifically, my laboratory discovered that the BAP1 gene is inactivated in 15% of clear-cell renal cell carcinomas. We found that BAP1 mutations are associated with high nuclear grade. That let us to hypothesize that patients who had BAP1 deficient tumors are going to have more aggressive tumors.
Furthermore, we found that mutations in BAP1 tended to anti-correlate with mutations in the second gene discovered by the Sanger Institute, by Michael Estrada and Andrew Futreal, the polybromo1 gene, PBRM1.
That led us to a classification that about 50% of the patients with clear-cell renal cell carcinoma will have PBRM1 deficient tumors and 15% of patients will have BAP1 deficient tumors. A small percentage of patients will have tumors that are deficient for both genes.
In a very productive collaboration we have had with Mayo Clinic, with Rick Joseph and Alex Parker, we’ve been able to determine that these different subtypes are associated with very different outcomes in patients. Patients that have tumors which are competent (not deficient) for both BAP1 and PBRM1 have excellent survival, whereas the cancer specific survival (CSS) is very poor in patients that have tumors that are deficient for both BAP1 and PBRM1. BAP1 deficient tumors have a somewhat intermediate survival phenotype, and the PBRM1 deficient tumors are similar to tumors that are competent for both BAP1 and PBRM1.
So we think for the first time, we’ve able to identify subtypes of clear-cell renal cell carcinoma that are likely to inform therapy in the future.
There is a gap between the discovery of the gene, to the determination of the clinical implications and subsequently to the therapeutic developments. That is because the therapeutic developments are going to emerge from the biologic understanding which we don’t have yet.
How can improved classification of kidney cancer subtypes improve clinical trial design?
That’s actually a very good question. So, what has traditionally happened is that a trial may be performed and one may find a group of patients–sometimes small, sometimes larger–that appear to do well with that agent. But if the group of patients is small, the trial is considered to be negative and the drug is abandoned. And I would say the problem is not that the drug did not have activity, it is that we were not able to identify the group of patients who appeared to benefit from that agent.
So the classification that we have developed and the identification of these different subtypes will pave the way to be able to do correlations. So then, when a clinical trial is executed when it is able to characterize better those subsets of patients that may benefit from the agent. For instance, as I was alluding to before, the BAP1 gene is inactivated in 15% of the tumors. It is possible that one of the drugs which has been tried in kidney cancer could have activity against that tumor. But there could never be a trial in that is positive that is being active in a small percentage of the patients, in 15% of the patients.
By identifying meaningful biological subtypes, we hope to deconvolute kidney cancer. It probably makes sense in trials going forward to do prespecified analysis of these genes that we now define as different biological subtypes–to be able to get at the question whether a particular treatment is having greater affect in one biological subtype versus the other. It is possible that it may not be that not all the PBRM1 deficient tumors that benefit, that are inhibited by a particular agent, there are other mutations. But it’s the beginning that which will lead us to identify those biomarkers and patients who are most resistant to a particular treatment.
What is the significance of improved disease classification for kidney cancer patients?
That is also an excellent question. These are discoveries that we and others have made over the last two or three years. The implications clinically have begun to be unraveled. It’s going to take significant effort and investment in research for us to go forward. We need to understand how loss of these genes, how mutations in BAP1 and PBRM1, are affecting processes inside the cancer cell, leading to kidney cancer development.
And in particular, we need to understand how BAP1, which is associated with most aggressive type of kidney cancer, is inducing that process. How is it that loss of the BAP1 gene makes the tumor be so aggressive? It’s only once we are able to elucidate the signaling pathways, that we will be able to identify targets for therapeutic invention.
On the other hand, we already know that for patients with localized disease, their prognosis is influenced biology of the tumor. I was alluding to this before, those patients who have removal of a tumor, localized to the kidney who deficient for BAP1 and PBRM1, they have a very high likelihood of recurrence in a short period of time. Those patients whose tumors are wild type for PBRM1 and BAP1 can do very well. (Wild type here means that the two genes are competent, or not deficient.)
Importantly, from the important view of translating these findings to the clinic, we have been able to develop assays, immunohistochemistry assays which are routinely performed in tumor samples at most institutions. (This is done in pathology labs).That allows us to very quickly determine whether we are dealing with the wild type tumor, BAP1 tumor, PBRM1 deficient tumor, or one that is deficient for both.
(Transcribed from the above YouTube video by Peggy Zuckerman. Any mistakes are mine alone, but hope this is helpful in understanding this approach to using gene sequencing in kidney cancer.
May 16, 2015)